Meet Your Physician: Dr. Robert Rolf
October 11, 2021
To read the full story in The Eagle, click here.
Beacon Orthopedics & Sports Medicine’s Robert Rolf, M.D. grew up in Cincinnati. He graduated from La Salle High School and then attended the University of Notre Dame where he earned a BS in Chemical Engineering.
When he was young, he was deeply and positively influenced by his uncle – a true father figure to him — Dr. Robert Burger, an orthopedic surgeon at Beacon Orthopedics. Dr. Burger is also a Notre Dame alum and always thought his nephew should attend medical school – and pursue orthopedics too. The young Robert wasn’t so sure.
As the son of two teenagers, he was the first in his family to graduate high school and attend college and had always been personally driven to succeed. Pursuing the engineering degree seemed a good fit and it was a great way into his early career. For two years after graduation he worked in engineering sales, however, the personal lure of becoming a physician was still inside him.
He turned his sights to medical school, attending the University of Cincinnati College of Medicine. At first, he was open to all specialties, but the more he studied and experienced, he kept being drawn to orthopaedics so that became his focus. “It seemed that the orthopedists I met and learned from (including my uncle) were well rounded – they were hardworking, athletic, committed to academic pursuits and still family centric,” Dr. Rolf said. “It just seemed a good fit for me too.”
Upon graduation from UC, Dr. Rolf completed his orthopaedic surgery residency at Emory University in Atlanta, Georgia. He continued his training as a shoulder and elbow specialist at the Boston Shoulder Institute at Harvard University. He is board-certified in orthopaedic surgery and holds a specialty certificate in Sports Medicine. He is the first to tell you that his practice is much more than simply treating athletes. “Shoulder pain can be debilitating,” he said. “And sometimes that pain needs the attention of an orthopedic specialist.” He shared that his goal is to help people live as pain-free as possible.
He has extensive training and years of experience in advanced arthroscopic techniques for shoulder instability and rotator cuff tears. He has also performed numerous complex shoulder reconstructive procedures such as total shoulder replacement and reverse shoulder replacement. He has truly become an expert.

Dr. Rolf relayed that he is most proud when his patients tell him that he’s “given them their lives back” – lessening or even eliminating their pain. Using his education, training and experience to help patients is what inspires him and in turn, his experience, personal training and dedication is inspirational to his patients. For athletes and non-athletes alike, that is a winning combination.
Beyond his patient service, Dr. Rolf is committed to helping future practitioners. One example of that commitment is his past role as the Co-Director of the Beacon Orthopaedics and Sports Medicine sports medicine fellowship program. This unique and highly competitive fellowship offers training to surgeons throughout the country about sports medicine and shoulder surgery. He hopes this work will be a positive influence on future practitioners. He wants to share what he experienced with is uncle and many other committed adults who took an interest in him throughout his youth and professional education and training.
“I truly have been blessed,” Dr. Rolf said. “My parents were only teenagers when they had me. My mother raised 3 boys on her own and never expected anything other than maximal effort.” He is a testament to knowing that hard work and dedication matter. Not only has it influenced his own career, but he purposefully shares that with all students he works with. “No matter what tough cards you’ve been dealt in life,” he said. “You can work to overcome obstacles and reach your goals.”
When not at work, he is with his wife and family. His free time is consumed happily with the interests and lives of their four active children.
If you are experiencing shoulder pain, contact Dr. Rolf or one of the more than 60 physicians at Beacon. Beacon Orthopaedics treats patients of all ages for various injuries and ailments – including shoulder difficulty. If you or someone you love is experiencing pain (whether from a sports injury or just usual exertion), you can always schedule a diagnostic appointment at one of the 20+ locations Beacon Orthopaedics has to offer in Greater Cincinnati.
Schedule an appointment 24/7 online or by calling 513-354-3700. More than twenty Beacon Tri-state locations are accepting new patients.
ASAP Podcast with Beacon Orthopedics Surgeon & Shoulder Specialist Robert Rolf M.D.
June 15, 2021
Robert Rolf M.D. is a native of Cincinnati, Ohio and a graduate of La Salle High School. He attended the University of Notre Dame where he received a BS in Chemical Engineering. This served as the foundation for furthering his studies into medicine and eventually, a specialty in the shoulder following his advanced research conducted at The Boston Shoulder Institute at Harvard under the guidance and fellowships with world reknowned shoulder surgeons. Nowadays, Dr.Rolf is the Co-Director of the Beacon Orthopaedics and Sports Medicine sports medicine fellowship program. He’s also a guest for our ASAP Podcast on the shoulder joint and rotator cuff.
The shoulder joint is definitely one of the more intricate joints of the human body. It’s an amazing structure, to say the least. And, it’s capable of some extraordinary athletic performance. USA gymnast, Simone Biles is not going to have extreme success performing a Yurchenko double pike without a the shoulder joint working to perfection. Quarterback Aaron Rogers would not be able to launch a football 70 yards with pinpoint accuracy with a seriously injured shoulder. Dr. Rolf, a distinctly skilled surgeon was able to share some of his time and expertise with ASAP~Athletic Stength And Power Podcasts in a discussion about the shoulder, and more specifically the rotator cuff, while making the intricasies of a very complicated joint quite easy to understand.
What is the rotator cuff?
The rotator cuff is a term used for a complicated area of the shoulder joint, comprised of tendons and relatively small musculature. The rotator cuff allows us to extend our arms up over our heads, rotate our shoulders, and throw a ball or object.
The main muscles that make up the rotator cuff are:
- the Supraspinatus
- the Infraspinatus
- the Teres Major
- the Subscapularis
Other important muscles in this region that need to be considered are the latissimus dorsi, the deltoids, the pectoralis muscles and the biceps and triceps. All of the aforementioned muscles play a key role in the function of the shoulder.
The shoulder, the rotator cuff and the muscles of the back are all interrelated with the large shoulder bone blades, or scapula, as well as the clavicle, humerus and acromion process. Interestingly, as Dr. Rolf discusses in our ASAP Podcast, there are seventeen muscles that attach to the scapula. Seventeen muscles! In addition, he explained that those smallish rotator cuff muscles are “two to four pound muscles”, meaning that two to four pound dumbells along with the exercise bands at The Bill Jacobs Power Company, are all that’s required to stimulate growth or repair to the area. The heavier weights used in bench pressing, vertical presses, cleans and rows are not effective in targeting the rotator cuff.
Athletes, especially those who are required to do a lot of throwing need to pay special attention to this area of the body. Career ending injuries or painful, nagging type injuries have been the demise of many athletes…both professional and amateur. Things can go wrong in this area….including, the aging process- where the shoulder slowly degrades over time, overuse injuries that lead to tendonitis, tears, impingement and sprains. Other injuries are due to muscle imbalances and also hard or heavy impact to the region.
A specialized program needs to be used to prevent injuries to the rotator cuff. This includes proper strengthening exercise and a regular flexibility program.
STRENGTH TRAINING for the Rotator Cuff
The following exercises should be included in a comprehensive program for the rotator cuff.
- Side lateral raises
- Side deltoid flys with a cable machine
- Front Deltoid Raises with a dumbell
- Rear deltoid flys (machine or dumbells)
- Dumbell Shoulder press on a inclined bench
- Lying “L” Flys
- Standing “L” Flys
- Lying Flys (arms straight out)
- Normal Grip Bench Press (avoid the wide grip technique!)
FLEXIBILITY PROGRAM
- Straight Armed Pectoralis Stretch
- Overhead Pole Stretch
- External Rotation Stretch
- Partner Deltoid Stretch
Schedule with Dr. Rolf online 24/7 by clicking here.
No, You Aren’t Too Young for Arthritis
May 12, 2021
And other facts about arthritis you should know
If you suffer from arthritis, you aren’t alone. More than 54 million adults in the United States live with doctor-diagnosed arthritis. The actual total of those who experience it could be almost double that number since most people don’t seek treatment until the pain is severe. In addition to the millions of adults suffering from it, nearly 300,000 children live with it, too.
By these estimates, more than 1 in 4 U.S. adults has some form of doctor-diagnosed arthritis. The estimate is even higher in rural areas where specialized healthcare access can be limited. The conservative estimate in those areas is 1 in 3 adults. In fact, it’s the top cause of disability in the United States. (Arthritis Foundation, 2020)
Orthopedics and Rheumatology
Arthritis can be treated by both orthopedists and rheumatologists.
- Orthopedists are surgeons who treat bone and joint diseases and injuries, such as arthritis, osteoarthritis and body trauma. They use varying care plan approaches depending on each patient’s unique situation — from medication to minimally invasive treatment and surgery.
- Rheumatologists are internal medicine physicians who focus on autoimmune conditions and non-surgical treatment of diseases like arthritis.
Could You Have Arthritis?
With any joint pain, there’s a chance arthritis could be the cause. Perhaps surprisingly, arthritis includes more than 100 types of joint-related diseases. The reasons can be varied but generally the sources include genetic predisposition, injury or illness that can lead to joint problems, or repetitive and/or stressful movements over time.
Prevention, as Always, is Key
You can’t fix genetics, and you also can’t change an injury or illness. You can, however, be aware of your risk factors and lead a healthy lifestyle to mitigate its potential effects.
If you believe your joint pain could be related to arthritis, early detection and putting a treatment plan in place are essential to slow progression of the disease and managing your pain. Your healthcare team can work together to help identify if you have arthritis and manage it if you do.
Diagnostic tests and physical exams are part of determining the root cause of your pain. Your Beacon physician will guide the development of an individualized care plan unique to your needs.
How is Arthritis Treated?
We, as orthopedists, look at arthritis treatment on three different levels: conservative, moderate, and surgery as the final option. We turn to surgery when your arthritis is no longer manageable with therapeutic and minimally invasive pain-management approaches.
Conservative: the sooner you seek medical attention, the longer conservative methods like the following have the potential to be effective. Treatments include:
- Anti-inflammatories
- Behavior modification
- Bracing
- Physical therapy
- Supplements
Moderate: If and when conservative measures aren’t able to help maintain your quality of life, there are moderate, minimally invasive treatments that can help manage pain, while still avoiding surgery. Those methods can include:
- Assistive devices
- Cortisone injections
- Hyaluronic acid injections
- Occupational therapy
Surgery: When all other approaches are failing, joint replacement surgery is typically the next recommendation. It is the only means currently available that can address and eliminate arthritis completely.
When It’s Time to See a Doctor for Arthritis Pain
At-home treatment that doesn’t improve your condition after a week
If you have minor ache and pain flare-ups, ice and heat, over-the-counter pain relievers and periods of rest can help. The Arthritis Foundation further suggests acupuncture, massage therapy, tai chi and yoga as a few options to help relieve arthritis pain. When you don’t notice improvements in your joint pain after a week of treating it with those methods, it’s time to see a doctor.
One of your joints goes rogue
You probably know your baseline of pain pretty well — as well as your body’s norms. If you start waking up with a swollen knee, wrist or other isolated joint, it may be cause for concern, and you should contact your doctor.
Rest doesn’t improve the pain
If you’ve been at rest or started resting for extended periods of time after joint pain and it doesn’t help, it’s time to see a doctor about starting or changing treatment.
Beacon Specialists are at the Ready
If you’d like to learn more about a pain that’s been keeping you from living your best quality of life, we’d love to help. We even have same-day appointments available. Schedule your appointment now to experience the Beacon difference.
Top Doctors 2020 at Beacon
January 15, 2020
Each year, physicians are selected by their peers in a survey, asking them which physicians they would turn to for their own personal care. Beacon doctors – 25 Tri-State physicians – were named to Cincinnati Magazine’s Top Docs List of 2020. We are very proud of all of our physicians and thank the medical community for their recommendations. Click on any of the physician’s names below to view their personal profile page, orthopedic specialty and discover why their peers view them as top doctors in the Cincinnati region.
You can schedule an appointment with our Board Certified and Fellowship Trained physicians online or by phone 24/7 with no referral necessary. Beacon has nine convenient locations, evening and weekend appointments and urgent orthopedic care clinics so that patients can get the care they need quickly.
Top Docs 2020:
Foot & Ankle Surgery
Hand Surgery
Orthopaedics Surgery
Pain Medicine
Physical Medicine & Rehabilitation
Spine Surgery
Sports Medicine
You can schedule with our physicians 24/7/365 online or by phone at (513)-354-3700.
What to Expect After AC Reconstruction
August 1, 2018
When we think of the shoulder joint, we often think of a single joint that allows us to raise or lower our arm, move it closer or further away from our body’s midline, or rotate it either internally or externally. The truth of the matter is that your shoulder relies on more than one joint. The “shoulder joint” consists of 4 joints: the glenohumeral joint, the acromioclavicular joint, the sternoclavicular joint, and the scapulothoracic joint. In order for the shoulder to have its full range of motion, these individual components must work together seamlessly.
As you would imagine, if any of these joints become severely damaged, the rest of the shoulder is affected. Unfortunately, shoulder injuries are common among athletes and other physically active individuals. Football players who take frequent blows to their shoulder, in particular, face a high risk of acromioclavicular joint separation. The acromonioclavicular joint, or AC joint, is located at the top of the shoulder and facilitates raising the arm over the head. When it is damaged, it can seem impossible to lift your arm, let alone reach overhead.
Not every AC injury requires surgery. However, if you are an athlete who needs to regain elbow function or if your symptoms impair your ability to live normally, an orthopaedic surgeon will recommend AC reconstruction. Reconstructive surgery is an option for both athletes as well as non-athletes to regain loss shoulder mobility. It is a standard procedure that has been shown to be highly effective. As with any form of surgery, though, your outcomes are determined in part by your adherence to post-operative guidelines. If you are considering reconstructive surgery, here is what you can expect during the months following your procedure and guidelines to follow in order to improve your outcomes.
Phase I – Immediate Post-Surgical Phase (Weeks 1 -4)
Rest should be your top priority following surgery. This will allow your shoulder to recover while also protecting it from further trauma. You can apply ice every hour for 15 minutes to minimize swelling and promote healing.
By the end of the fourth week, you should be able to passively bend your arm and move it away from the midline of your body by 70 degrees. A passive range of motion refers to someone else—such as a physical therapist—moving the joint for you. By contrast, active range of motion refers to your ability to move your joint on your own.
Goals:
- Minimize shoulder pain and inflammatory response
- Protect the integrity of the surgical repair
- Achieve gradual restoration of passive range of motion
What to Expect:
- Minimal pain which will gradually decrease
- No active range of motion in the affected shoulder
- Gradual restoration of passive range of motion
- Use of a sling for the first 4 weeks
- The need for assistance in order to complete daily activities
- Physical therapy starting at week 2
- Education regarding posture, joint protection, positioning, etc.
Milestones to Progress to Phase II:
- Appropriate healing of the surgical repair
- Adherence to the post-operative protocols
- Achieved at least:
- 90 degrees of passive forward elevation
- 30 degrees of passive external rotation at 20 degrees abduction
- 30 degrees of passive internal rotation
- Completion of Phase I activities without pain or difficulty
Phase II – Intermediate Phase (Weeks 4 – 8)
Goals:
- Continue to minimize shoulder pain and inflammatory response
- Continue to protect the integrity of the surgical repair
- Continue to restore passive range of motion
- Achieve gradual restoration of active range of motion
- Discontinue use of the sling by the end of week 6-8
What to Expect:
- Minimal to no pain and inflammation
- Discontinued use of a sling
- Continued physical therapy
- Gradual restoration of passive range of motion
- Gradual restoration of active range of motion starting at week 8
- Continued education regarding posture, joint protection, positioning, etc.
Milestones to Progress to Phase III:
- Achieved at least:
- Passive forward elevation at 165 degrees
- Passive external rotation at least 75 degrees at 90 degrees abduction
- Passive internal rotation at least 50 degrees att90 degrees abduction
- Active forward elevation at lest 145 degrees with good mechanics
- Dynamic control of the scapula (shoulder blade)
- Appropriate posture of the scapula (shoulder blade) at rest
- Completion of Phase II activities without pain or difficulty
Phase III – Early Strengthening Phase (Weeks 10 – 16)
Goals:
- Initiate balanced strengthening program
- Normalize strength, endurance, and neuromuscular control
- Resume chest level full functional activities
- Strengthen scapular retractors and upward rotators
What to Expect:
- Pain-free activities
- Continued physical therapy:
- Exercises requiring progressively greater intensity, shoulder elevation and joint stress
- Exercises consisting of both open chain and closed chain activities
- No heavy lifting or plyometrics
- Continued education regarding posture, joint protection, positioning, etc.
Milestones to Progress to Phase IV:
- Achieved passive forward elevation within normal limits
- Achieved external rotation at all angles of abduction within normal limits
- Active forward elevation within normal limits with good mechanics
- Appropriate rotator cuff and scapular muscular performance for chest level activities
- Completion of Phase III activities without pain or difficulty
Phase IV – Return to Activity Phase (Approx. Week 24)
Goals:
- Continue stretching and passive range of motion as needed
- Continue all exercises from the aforementioned phases
- Maintain full non-painful active range of motion
- Return to full strenuous work activities
- Return to full recreational activities
What to Expect:
Heavy weight lifting and overhead athletic moves should resume 6 months following your operation or after being cleared by an orthopaedic specialist.
Speak with an Orthopaedic Specialist
Your adherence to post-operative guidelines following AC reconstruction directly impacts your outcomes. And while the importance of rehabilitation cannot be stressed enough, it is important to also understand that it is only one half of the equation. Both your recovery program as well as your choice of orthopaedic surgeon will ultimately determine the success of your joint reconstruction.
Dr. Robert Rolf is a board certified orthopaedic surgeon at Beacon Orthopaedics and Sports Medicine who provides extensive expertise in rotator cuff tears as well as other conditions related to the shoulder or elbow. For your convenience, Dr. Rolf meets with patients at Beacon’s Batesville, Lawrenceburg, or Northern Kentucky locations as well as Beacon West in Harrison, Ohio. Schedule an appointment online to meet with Dr. Rolf.
Total Shoulder Replacement or Reverse Shoulder Replacement
July 30, 2018
Total Shoulder Replacement or Reverse Shoulder Replacement
Shoulder arthroplasty, often called a total shoulder replacement, is a well-established surgery for treating severe pain and stiffness. In fact, approximately 53,000 people in the U.S. have shoulder replacement surgery each year in order to regain comfort and function, according to the Agency for Healthcare Research and Quality. And while the majority of these procedures would be considered standard replacements, patients may be surprised to know that a “reverse” replacement is also an option. In some situations, a reverse shoulder replacement may benefit a patient more than a standard procedure.
At Beacon Orthopaedics and Sports Medicine, our shoulder specialists have performed numerous total shoulder replacements and reverse shoulder replacements. If you are experiencing shoulder pain and stiffness that limits your activities during the day and keeps you awake at night, you should talk to a specialist about your options. Here is information about total shoulder replacements and reverse shoulder replacements to help guide your discussion.
Q: What is a total shoulder replacement?
In a healthy shoulder, the head of the upper arm bone (humerus) fits into a shallow socket in the scapula. In shoulder replacement surgery the damaged portion of the humerus is removed and replaced with a smooth metal ball attached to a stem. This artificial component, called a prothesis, will either replace the “ball” of the joint or both the “ball” and “socket.”
Q: What is a reverse shoulder replacement?
In reverse shoulder replacement surgery, the damaged portions of the shoulder are also replaced with a prosthesis made from metal and plastic. However, unlike a standard replacement, the artificial component is placed on the socket side of the joint. The socket is then placed on the arm side where it is supported by a metal stem. Thus, the prosthesis is reverse of where its natural counterparts would be located within the body.
Reverse shoulder replacement works best for patients with cuff tear arthropathy or a detached rotator cuff. The reverse prosthesis allows the patient to use their deltoid muscles instead of their deteriorated or detached rotator cuff tendons in order to lift their arm.
Q: What are the benefits of shoulder replacement surgery?
First and foremost, the purpose of shoulder surgery is to relieve chronic pain and restore mobility so patients can resume normal living. Additionally, an orthopaedic surgeon may recommend a shoulder replacement in order to treat the following conditions:
- Osteoarthritis
- Rheumatoid Arthritis
- Post-traumatic Arthritis
- Rotator Cuff Tear Arthropathy
- Avascular Necrosis
- Severe Fractures
- Bone Tumors
In recent years, advancements in prosthetic designs have allowed patients to resume active lifestyles following surgery. Patients can often return to baseball, golf, swimming, or many of the other activities they enjoy.
Q: How successful is shoulder replacement surgery?
Both total shoulder replacement and reverse shoulder replacement have been shown to be highly effective. As with all forms of surgery, however, the effectiveness of the procedure depends on the overall health of the patient, their participation in physical therapy, and the expertise of the orthopaedic surgeon. Patients can improve their outcomes by choosing an experienced orthopaedic surgeon and adhering to their treatment plan.
Q: What are the potential risks of shoulder surgery?
Shoulder replacements are considered as safe as hip and knee replacement surgeries. Of course, as with any joint replacement surgery, there are associated risks. The most common complication is the dislocation of the prosthesis, with dislocations being more likely to occur among reverse shoulder replacements. Fortunately, a dislocation can be managed by placing the arm back into the proper location and keeping the arm immobile for a period of time.
Shoulder replacement surgery also carries risks associated with other forms of surgery, including:
- Infection
- Fracture
- Nerve or blood vessel damage
- Joint stiffness or instability
- Loosening of the prothesis
- Dislocation
Although rare, other complications may occur. An experienced orthopaedic surgeon can talk to you about these complications and discuss your individual level of risk. In some instances, additional surgery may also be necessary.
Q: How long does it take to recover from shoulder surgery?
For the first 7-14 days following surgery, you will need someone to assist you with your daily activities at home as well as transportation. You should also expect your arm to be in a sling for the first 3-6 weeks and to participate in physical therapy for the first 8-12 weeks.
After about 6 weeks following your surgery, you may resume driving with the permission of your surgeon. You may also be cleared to return to work depending on how much physical activity is required.
After 1-2 months you may resume lifting heavier objects above the shoulder level.
For most patients, shoulder surgery typically requires 3-6 months for a full recovery.
Q: Who is a candidate for shoulder replacement surgery?
The typical shoulder replacement patient is 60-80 years old. It’s important to note, however, that younger patients may also require surgery. Candidates for total shoulder replacements typically have debilitating, chronic pain or severely restricted joint mobility that interferes with daily activities. And while severe osteoarthritis, rheumatoid arthritis, or another form of the disease are common among patients, shoulder arthritis is not the only condition that may require surgery in order to treat.
Is Shoulder Replacement Appropriate for You?
Every patient’s situation is different and an experienced orthopaedic surgeon whether a total shoulder replacement or reverse shoulder replacement is appropriate for you. If you experience chronic pain and have not achieved relief with conservative, non-surgical treatments, contact Beacon Orthopaedics and Sports Medicine today to schedule an appointment with Dr. Rolf.
Rotator Cuff Tear and Surgery
July 24, 2018
In this article, the experts at Beacon Orthopaedics explore the range of symptoms involved with rotator cuff tears, the necessary treatments to relieve patient symptoms—and, more specifically, the benefits of pursuing Superior Capsular Reconstruction using allografts to repair irreparable rotator cuff tears versus the more common treatment options.
The Rotator Cuff and Shoulder Stability

Your shoulder joint is the most mobile joint in your body. However, no matter the level of mobility within the shoulder, its lack of strong ligaments leaves your shoulder reliant on its surrounding muscles to maintain stability—in which your rotator cuff plays a critical role.
Rotator cuff tears are common, at times hard to detect, and among the more difficult injuries to treat.
When it comes to properly treating rotator cuff tears, physicians make their diagnosis on a per-patient basis. Symptoms vary between patients:
- Some experience severe shoulder weakness and are unable to raise their arm
- Some experience pain over the top of the shoulder but can still raise their arm
- Some experience no pain and experience functional limitations of the arm
- Some experience pain that descends down the arm—sometimes even down to the elbow
However, once diagnosis is reached, the path to recovery is still uncertain. In most cases, physicians first suggest non-surgical treatments for rotator cuff repairs, such as physical therapy, anti-inflammatory medications, or cortisone injections, because surgical treatments have a higher likelihood of either causing more damage to the torn tendons, or need of a revision surgery over time.
Before surgical treatments are planned for patients, your physician must discuss the following to be sure surgery is the best option:
- Your past and current symptoms
- Damages due to your rotator cuff tear
- Size and location of your tear
- Your activity level
- And all other treatments that have been attempted in your case
Solutions for Irreparable Rotator Cuff Tears
Shoulder functionality with an irreparable rotator cuff tear ranges from little to none.
Rotator cuff injuries—where the tendons at the ends of the rotator cuff muscles become torn and result in pain and limited shoulder mobility—frequently occur following a trauma to the shoulder joint or through general wear and tear on tendons within the rotator cuff over time.
If the tendons tear chronically, the connected muscle involutes and is replaced by fat and scar tissue, making the muscle too stiff to contract with enough force to rotate the humeral head on the socket effectively—resulting in restricted shoulder mobility.
When conservative measures fail and patients continue to experience pain, surgery is the next logical step. However, patients diagnosed with irreparable rotator cuff tears are typically met with very limited options for treatment.
Surgical procedures such as reverse shoulder replacement—where the ball and socket structure of the shoulder joint is reversed—don’t fully address the problem faced by patients with irreparable rotator cuff tears. Even though this procedure reverses which muscles support shoulder stability, shifting from the rotator cuff muscles to the deltoid muscles, this method often leads to required revision surgeries down the line for some patients.
Arthroscopic SCR using Allografts as an Alternative Solution for Irreparable Tears
Dr. Rolf at Beacon Orthopaedics, performs arthroscopic superior capsular reconstructions using allografts as an alternative surgical procedure to aid in shoulder stability and improve shoulder function despite the occurrence of irreparable rotator cuff tears.
Superior Capsular Reconstruction (SCR)—an arthroscopic procedure where a graft is secured to the glenoid and greater tuberosity—makes use of allografts to strengthen and reconstruct the superior capsule to ensure that patients regain the ability to maintain the natural mechanics of the shoulder.
What is an Allograft?
An allograft is tissue taken from one person for transplantation into another—including bone, tendons, ligaments, skin and heart valves. Donation is always voluntary and requires consent, from either the donor in question before death or the donor’s family post-mortem. After authorized consent is obtained, potential donors are thoroughly screened for risk factors and medical conditions that would rule out donation.
Procedures where allografts are used:
- Shoulder repair
- ACL repair
- Joint reconstruction in the knee and ankle
- Meniscal replacement
- Reconstruction due to cancer or trauma
- Ridge augmentation in dental procedures
- Spinal fusion
- Urological procedures
Why Use Allografts?
The preference of allografts over autografts is the ability to keep the treatment limited to one surgery versus requiring two. When surgeons use an allograft, it is already pre-screened for risk factors, so there is no need to retrieve a graft from another part of your body, and get that autograft ready to use for your procedure.
When receiving an allograft implant, be sure to ask your surgeon about tissue preparation and sterilization.
Currently Experiencing Shoulder Pain or Instability?
Consult a physician now. Dr. Robert Rolf, one of the physicians at Beacon Orthopaedics and Sports Medicine, received extensive training in advanced arthroscopic techniques for shoulder instability and rotator cuff tears and has world class experience in complex shoulder reconstructive procedures including tendon transfers, shoulder replacement, and reverse shoulder replacement procedures. If you are reading this article to figure out if you might have a rotator cuff tear, or are unsure of which treatment method might be best for the specific symptoms you’re experiencing, scheduling an appointment with Dr. Rolf will provide more information for your particular case.
Frequently Asked Questions: AC Joint Injuries
July 24, 2018
AC joint injuries are common among those who participate in competitive athletics. Two of the most common ways people injure their AC joint is by falling on an outstretched arm or running directly into something.
In this article, Dr. Robert Rolf of Beacon Orthopaedics and Sports Medicine will explore AC joint injuries and some of the most frequently asked questions by patients. If you are experiencing any of the symptoms discussed in this article, schedule an appointment today.
What is the AC joint, and what symptoms should I look for to know it’s an AC joint injury?
Your shoulder is formed at the junction of the clavicle, the scapula, and the humerus. The joint between the end of the scapula (the acromion) and the clavicle is called the acromioclavicular joint (AC joint)—one of the important functional joints that allows a full range of movement in the shoulder joint held together by three ligaments which are acromioclavicular, coracoclavicular, and the coracoacromial ligaments.
Some of the signs and symptoms of AC injury are:
- Pain on the top of the shoulder
- Pain when lying on the involved side
- Pain increases with heavy lifting or overhead and across body movements
- Swelling and bruising along the shoulder
- Tenderness over the AC joint
- Decreased range of motion and stability
- Decreased strength
- A visible bump on the top of the shoulder
- A popping sound or catching sensation
What are the Most Common Causes of AC Joint Pain?
Chronic irritation from repetitive overhead motions:
- Baseball
- Weightlifting
- Volleyball
- Basketball
Contact sports with high-risk for falls and collisions:
- Football
- Wrestling
- Rugby
- Biking
- Snow sports
- Hockey
What are the different types of AC joint injuries?
Type I: where the force applied to the acromioclavicular and coracoclavicular ligaments is too mild to tear them. This will result in only a sprain of the AC joint, and will hurt but not show any evidence of an acromioclavicular joint dislocation.
Type II: where heavier force is applied to the shoulder—disrupting the AC ligaments but leaving the coracoclavicular ligaments intact (but sprained). When these injuries occur, the lateral clavicle becomes more prominent.
Type III: where the force applied to the shoulder completely disrupts the AC ligaments and coracoclavicular ligaments—leading to complete separation of the clavicle and the resulting protrusion or “bump.”
Type IV: where there is posterior displacement of the clavicle, buttonholing through the trapezius muscle.
Type V: where the clavicle is widely displaced as a result of disruption of muscle attachments.
Type VI (rare): where there is inferior displacement of the distal clavicle below the acromial process or the coracoid process.
Can Physical Therapy Help?
Once an AC joint injury is officially diagnosed, your physician will work with you to develop an individualized plan of action to start your recovery. Most patients with AC joint injuries will start to feel better within a few days or a week of the injury—but it can take at least six weeks for the AC ligaments to fully heal. During that time, it’s crucial to take the pressure off of the AC joint to protect from overstretching the immature scar tissue. While it’s helpful to use a sling, tape or a shoulder brace to de-load your AC joint, physical therapy will be the key to most AC joint injury recovery plans.
Physical Therapy Treatment Goals for AC Joint Injury:
- Range of Motion – regain ability to move without pain.
- Strength Training – regain the strength in the shoulder to better prevent re-injury.
- Pain Management – reduce the amount of residual pain as you go about your normal activities.
- Functional Training – increase your ability to move your shoulder correctly without putting undue pressure on your AC joint.
Who Should I Talk to About My Recovery Options?
Dr. Rolf of Beacon Orthopaedics received extensive training in advanced arthroscopic techniques and world-class experience in complex shoulder reconstructive procedures for tendon transfers, shoulder replacement, and reverse shoulder replacement procedures. If you think you might have sustained an AC joint injury, schedule an appointment today to speak with Dr. Rolf about your options. His experience and passion for sports medicine will ensure that you return to your favorite activities stronger and better than ever.
Is My Shoulder Pain from Arthritis or Bursitis?
June 14, 2018
Your shoulders are packed with bones, muscles, tendons, and ligaments. Shoulder pain can develop from a variety of conditions that affect one—if not many—of these structures. While this can make it difficult to pinpoint the exact source of your shoulder pain, an accurate diagnosis and proper treatment are the key to recovery.
Arthritis and bursitis are two of the most common causes of shoulder pain; however, they can be difficult to differentiate. The following article will help you determine if your shoulder pain is caused by arthritis or bursitis.
What is Shoulder Arthritis?
Arthritis is derived from the Greek word, “arthron”, which means joint and the Latin suffix “itis”, meaning inflammation. In the past, arthritis was defined by inflammation in one or more of the body’s joints. Today, arthritis has come to describe any disease that wears away cartilage, which is the smooth tissue that covers the ends of bones where they meet and reduces friction. Arthritis affects not only joints, but also muscles, tendons, and ligaments.
The three most common forms of shoulder arthritis are: osteoarthritis, which is a degenerative joint disease; post-traumatic arthritis, which is a disease that results from an injury; and rheumatoid arthritis, which is an autoimmune disease. Joint pain and limited range of motion are characteristic of every form of the disease. Additional symptoms will depend on the exact type of arthritis affecting your shoulder.
Symptoms of Shoulder Arthritis
Shoulder arthritis may cause any of the following symptoms:
- Shoulder pain that gradually becomes worse with time
- Shoulder pain that becomes worse after a period of inactivity (e.g. sleep)
- Shoulder pain with certain motions (e.g. reaching overhead)
- Shoulder tenderness and sensitivity to pressure
- Shoulder stiffness or loss of motion
- Swelling in the shoulder joint
- Muscle weakness in the shoulder
- Popping, crunching, or catching sensation in the shoulder
Osteoarthritis
Osteoarthritis—sometimes called “wear and tear arthritis” or degenerative joint disease—is the form of arthritis that is most likely to affect the shoulder, in addition to being the most common chronic joint condition overall. It is a degenerative condition that destroys the smooth articular cartilage of the shoulder, leading to pain, swelling, and immobility. In the final stages of osteoarthritis, cartilage is fully worn away and bone rubs against bone.
The risk for osteoarthritis rises steeply after age 50 in men and age 40 in women. Repetitive, occupation-related injury and physical shoulder trauma can also contribute to the development of the disease. And, as with other forms of arthritis, genetics play an important role in the development of osteoarthritis.
Post-Traumatic Arthritis
Post-traumatic arthritis is a specific form of osteoarthritis that may occur if cartilage is damaged during an injury. Sports, military, or automobile accidents can all lead to the type of injuries that result in post-traumatic arthritis; however, so can a fall or a traumatic blow to the shoulder. Chronic overuse of the shoulder as well as excess body weight can also accelerate the progression of the disease.
Rheumatoid Arthritis
Rheumatoid arthritis is an autoimmune disease that occurs when the body’s immune system mistakenly attacks the synovium membrane, which lines the cavities of joints and other structures. If left untreated, rheumatoid arthritis will eventually damage adjacent cartilage and bone, resulting in pain, swelling, inflammation, and loss of function. It is also symmetrical, meaning that it usually affects both shoulders.
It is important to note that rheumatoid arthritis can develop, progress, and worsen with minimal or no apparent symptoms. Moreover, because characteristics of the rheumatoid arthritis overlap with other conditions, it is possible for it to be misdiagnosed, allowing the disease to progress further and delaying the appropriate treatment.
What is Shoulder Bursitis?
Bursitis occurs when the bursa, a fluid-filled sac that protects the outside of a joint, becomes inflamed. While it can be caused by acute trauma to the shoulder, it is more likely to result from chronic overuse of the joint. Moreover, because the structures of the shoulder are closely packed together, inflammation that begins in one of the five bursae in joint will eventually impact the others. Therefore, shoulder bursitis is often not only the result of an injury but also likely to create additional complications.
Symptoms of Shoulder Bursitis
Shoulder bursitis may cause any of the following symptoms:
- Shoulder pain located at the top and outside of the joint
- Shoulder pain that is triggered by movement or repetitive motion
- Shoulder pain that gradually becomes worse
- Shoulder tenderness and sensitivity to pressure
- Shoulder redness and warmth
- Muscle weakness in the shoulder
- Fever (if caused by an infection)
The subacromial bursa is the largest bursa in the body and is highly susceptible to bursitis. It is located below the acromion, the large bony projection on the scapula (shoulder blade). This is why the majority of pain associated with shoulder bursitis occurs at the top and outside of the joint and radiates down the arm. It should also be noted that, although bursitis is the result of inflamed soft tissue, visible swelling is rare. Shoulder bursae do not have to be much thicker than normal to cause pain and so it is unlikely that you will have any visible signs aside from some minor redness.
Athletes, first and foremost, face the greatest risk of developing bursitis. This is particularly true of baseball pitchers, tennis players, and swimmers. Their greater than average risk is the result of not only their activities on the field but also from hours of repetitive, physically demanding training all year round. Moreover, the risk of bursitis is not limited to collegiate and professional athletes. Rapid growth, decreased flexibility, training errors, and overspecialization in one sport or activity can also contribute to a young athlete’s risk of developing bursitis.
Manual laborers, especially those who use their shoulder to perform overhead motions, are also prone to develop bursitis. This includes, but is not limited to, construction workers, factory workers, and painters.
Even hobbies and household chores can lead to bursitis if the shoulder is not given adequate rest. Examples include cleaning, gardening, and hanging clothes to dry. It is important to take note of what activities at home involve your shoulder and make an effort to space them apart.
Is it Arthritis or Bursitis?
In the most general sense, arthritis is a long-lasting condition that affects bones and cartilage while bursitis is a transient condition that affects bursae, tendons, ligaments, and muscles.
Arthritis |
Bursitis |
|
|
|
|
|
|
|
|
|
|
Talk to a Shoulder Specialist
Dr. Robert Rolf is a board-certified shoulder specialist at Beacon Orthopaedics and Sports Medicine who can accurately diagnose your shoulder pain as arthritis or bursitis. He will talk to you about your symptoms, perform a comprehensive physical examination, and prescribe the appropriate treatment. You can schedule an appointment online to meet with Dr. Rolf.
Shoulder Trauma and Recovery: Fractures
June 13, 2018
 Shoulder pain is far too common. Unfortunately, the discomfort of a stiff, painful shoulder is often made worse by the frustration of pinpointing its exact cause. The shoulder can be injured in a variety of ways, including dislocations, labral tears, rotator cuff tears, rotator cuff tendonitis, shoulder impingement, frozen shoulder, and shoulder osteoarthritis. This article will focus on shoulder fractures and will help you determine if your pain is caused by a broken bone.
Shoulder pain is far too common. Unfortunately, the discomfort of a stiff, painful shoulder is often made worse by the frustration of pinpointing its exact cause. The shoulder can be injured in a variety of ways, including dislocations, labral tears, rotator cuff tears, rotator cuff tendonitis, shoulder impingement, frozen shoulder, and shoulder osteoarthritis. This article will focus on shoulder fractures and will help you determine if your pain is caused by a broken bone.
It is important to keep in mind that only an orthopaedic specialist can diagnose your pain. Schedule an appointment with a shoulder specialist for an accurate diagnosis and comprehensive treatment.
Anatomy of the Shoulder
The shoulder is made up of 3 bones, including:
- The clavicle (collarbone) which is a long, thin bone that begins at the base of the neck and continues to the shoulder.
- The humerus (upper arm bone) which runs from the shoulder to the elbow.
- The scapula (shoulder blade) which is a triangle-shaped bone that connects the clavicle and humerus.
Shoulder fractures can affect any of these bones as well as nearby muscles, ligaments, and tendons.
Shoulder Fractures
Types of Shoulder Fractures
A fracture is a broken bone. It can range from a small crack, also known as a hairline fracture or a stress fracture, to a complete break in the bone. Breaks can occur in any of the three shoulder bones:
- Clavicle fractures are a common type of shoulder fracture. A break in the collarbone commonly occurs when a person falls on their shoulder or with their arm stretched out. A clavicle fracture is also typically associated with a bump or protrusion.
- Humerus fractures are also a common type of shoulder fracture. A break in the humerus is classified as either proximal humeral fractures or humerus shaft fractures based on whether the break occurs close to the shoulder joint or in middle portion of the bone respectively. A break in the humerus is often the result of a high-energy event, such as a direct blow to the shoulder or a traumatic motor vehicle accident. Proximal humeral fractures, in particular, are also common among the elderly who are suffering from osteoporosis
- Scapula fractures are very rare. This is primarily due to the joint’s mobility and the thick layers of muscles surrounding the bone. A heavy, blunt force—such as a high-speed vehicular accident or a fall from a great height—is typically required to break the scapula.
Moreover, fractures are described as either displaced or non-displaced. The majority of shoulder fractures are non-displaced, meaning that the bone fragments remain near their correct anatomic position. Displaced fractures, however, require a physician to manipulate the bone back to the correct position.
Symptoms of Shoulder Fractures
All shoulder fractures involve one or more of the following symptoms:
- Severe pain that often becomes worse with arm movement
- Swelling or bruising at the fracture site
- Deformity (such as a bump or protrusion) at the fracture site
- Inability to move the arm
- Grinding sensation when moving the shoulder
Complications Caused by Shoulder Fractures
The most common complications caused by shoulder fractures are:
- Poor shoulder function or immobilization occurs when the arm is unable to move through its full range of motion.
- Shoulder stiffness develops due to the limited movement following a fracture.
- Post-traumatic arthritis is a specific form of osteoarthritis that results from injury. Arthritis will continue to cause pain, swelling, stiffness, tenderness, and joint instability long after the fracture has healed.
Complications related to bone healing and alignment may also occur. These include:
- Malunion occurs when a bone heals in the wrong position.
- Delayed union refers to a fracture that takes longer than usual to heal.
- Nonunion refers to a fracture that fails to heal.
Inadequate immobilization of the shoulder, blood supply, and nutrition all contribute to a patient’s risk for these conditions. Use of tobacco or nicotine can further inhibit bone healing and increase a patient’s risk for complications.
It’s also important to understand that all fractures damage nerves, blood vessels, and soft tissue. Rotator cuff tears occasionally occur at the same time as a fracture. And, although rare, diminished blood supply to bones can lead to a serious, life-threatening complication called avascular necrosis. Avascular necrosis, also called osteonecrosis or aseptic necrosis, causes bones to become painful, weak, and eventually collapse. These conditions can further complicate a fracture and should be treated early.
Treatments for Shoulder Fractures
Conservative treatments are used to treat shoulder fractures, regardless of their severity. These treatments include:
- Immobilization to keep bone fragments together and in the correct anatomical position. A physician will typically recommend a sling, splint, or cast for 2 to 4 weeks. An immobilization device may be recommended for longer, depending on the location and severity of the fracture.
- Physical Therapy helps restore shoulder motion and strength. Physical therapy typically starts 2 to 3 weeks after the injury occurs.
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) are used to relieve mild to moderately severe pain.
Many shoulder fractures heal in approximately four months with non-surgical treatment; however, some shoulder fractures require surgery in order to heal properly. Minimally-invasive shoulder fracture repair and shoulder replacement surgery are effective options for treating severe breaks and many possible complications.
Talk to a Shoulder Specialist
If you are experiencing pain in your shoulder, ask yourself these questions:
- Are you able to move your arm through its full range of motion?
- Are you able to successfully perform normal, everyday activities with your shoulder?
- Do you experience a sharp pain in your shoulder?
- Does the pain increase with movement?
- Does the pain persist through the night?
- Do you experience a grinding sensation in your shoulder?
- Do you notice an obvious deformity in your arm or shoulder?
These are signs of a serious shoulder injury.
Schedule an appointment with Dr. Robert Rolf if you are concerned that you may have a shoulder fracture. Dr. Rolf is a board-certified orthopaedic surgeon at Beacon Orthopaedics & Sports Medicine with expertise in shoulder reconstruction and replacement. Patients can meet with Dr. Rolf at Beacon’s Batesville, Lawrenceburg, or Northern Kentucky location as well as Beacon West in Harrision, Ohio. Dr. Rolf also offers Shoulder Talks at Beacon West. Visit Dr. Rolf’s page for more information on his free shoulder talk seminars or to schedule an appointment today.
Total Shoulder Replacement Recovery Plan
June 13, 2018
Total shoulder replacement surgery, also known as total shoulder arthroplasty, is an effective way of treating permanent joint damage caused by arthritis. It can relieve the severe pain and stiffness in a patient’s shoulder and allow them to return to sports they enjoy such as baseball, golf, or swimming.
While the long-term benefits of a shoulder replacement cannot be overstated, patients must also consider how a replacement will affect them during the months immediately following their procedure. Recovery does not happen overnight—it’s a gradual process. Patients must be willing to limit or modify their activities as they slowly regain shoulder strength and mobility. Moreover, participating in physical therapy will not only help ease shoulder pain and help restore shoulder function in the short-term, but it will also help the patient preserve their new joint for years to come.
This article provides general recovery guidelines for shoulder replacement surgery. It is important to note, however, that there are many types of shoulder replacement surgery, including:
- Total shoulder replacement (traditional shoulder arthroplasty)
- Reverse shoulder replacement (reverse total shoulder arthroplasty)
- Partial shoulder replacement (stemmed hemiarthroplasty)
- Shoulder resurfacing (resurfacing hemiarthroplasty).
The recovery guidelines that you will be expected to follow may vary based on the type of surgery you receive. For a detailed explanation of what you can expect, talk to a shoulder specialist.
Before Surgery
The majority of your recovery period will be spent at home. At Beacon Orthopaedics and Sports Medicine, total shoulder replacement is performed in an outpatient setting so patients return home even sooner. Since you will not be able to use your arm for several weeks, making preparations at home will make the recovery process a little smoother.
Equipment and Supplies
Take note of activities in your daily routine that require the use of your arm and plan accordingly. It is highly recommended that patients of total shoulder replacement surgery have:
- Detachable showerhead. You will need to keep your incision dry so a detachable showerhead is helpful. Moreover, you may consider a large waterproof bandage or a second sling that you can leave to dry between showers.
- Many patients find it helpful to sleep in a reclined position because it puts less strain on the shoulder. This can be achieved by bolstering your lower and mid back with pillows. You may also find it comfortable to prop your injured up on a pillow while sitting.
- Packaged or frozen food. You should continue to eat fresh meals when possible; however, having packaged or frozen food provides you with convenient options.
- Clothes that button or zip. Having clothes that you can button or zip, instead of pulling over your head, will make dressing a lot easier.
- Velcro strap shoes. Tying shoelaces with only one hand is inconvenient. Consider shoes that you can easily slip on and off.
In general, you should stock up on supplies that you use regularly. Most patients cannot drive for 6 to 8 weeks after surgery, so you may need to depend on others when supplies are low.
Assistance and Monitoring
Identify several family members and friends who will assist you during your recovery. These individuals will help you around the house and drive you where you need to go for the first several weeks after surgery. Expect to need a lot of assistance on both the day of your surgery as well as the immediate days following it, and gradually need less as you return to normal shoulder function.
After Surgery
Incision Care
Keep the bandage over your wound clean and dry. Your physician may restrict you from taking a shower for the first few days after your surgery; however, you may be advised to change the bandage every day. Do not shower until your physician gives you permission. When you do, let the water run over the incision and do not scrub.
Contact your physician immediately if you experience any of the following:
- Bleeding that soaks through your bandage and does not stop with applied pressure.
- Pain that does not go away with pain medicine.
- Moving or shifting in your new shoulder joint.
- Temperature higher than 101°F (38.3°C). This is a possible sign of an infection.
- Tenderness, redness, or pain in your calf, chest pain, and/or shortness of breath. These are all signs of a possible blood clot.
Precautions and Physical Therapy
In order to ensure a fast recovery and the best possible outcome, it is imperative that you adhere to the recovery plan outlined by your physician. The plan will include precautions to help protect your new joint as well as physical therapy to restore shoulder strength and mobility.
Recovery is a gradual process. Typically, it takes at least 4 – 6 months for a patient to return to their pre-injury level of activity. In some cases, it may take as long as 9 – 12 months to make a full recovery. In either case, it is important that you maintain realistic expectations about your progress. The following is a general recovery timeline for total shoulder replacement surgery. For a more specific timeline, see Dr. Rolf’s list of physical therapy protocols.
Phase I: Immediate Post-Surgical Phase (Weeks 1 – 4)
Precaution: Prevent the arm from moving with use of a sling
Your arm will continuously be in a sling for approximately the first four weeks following surgery. Always use the sling when you are walking or standing. If you are sitting or lying down, you can use a pillow to support your arm. You will gradually use your sling less as you near the end of the phase.
Precaution: No lifting or weight-bearing on the operated arm
During this phase, you will have no active range of motion (AROM) in your shoulder. In other words, you will not be able to move your shoulder on your own. At this time, a physical therapist will also begin working with you to restore passive range of motion (PROM) in your shoulder. PROM refers to your ability to move your shoulder with assistance.
Phase II: Early Strengthening Phase (Weeks 4 – 6)
Precaution: No heavy lifting or weight-bearing on the operated arm
Precaution: No sudden jerking movements in the operated arm
Your physical therapist will also begin exercises with you to gradually restore AROM in your shoulder. Typically, patients can lift objects no heavier than a coffee cup by this point.
Phase III: Moderate Strengthening Phase (Post-6 Weeks)
Precaution: No heavy lifting in excess of 5 lbs. with the operated arm
Precaution: No sudden jerking movements in the operated arm
Your physical therapist will continue to work with you to focus on gradually increasing shoulder strength, endurance, and functional mobility.
Phase IV: Advanced Strengthening Phase (Post-12 Weeks)
Precaution: Ensure gradual progression of shoulder strength
You should continue to exercise 3 – 5 times a week. At Beacon Orthopaedics, a physical therapist can create a customized routine of sport-specific training exercises for you. This will include ways to preserve your new joint for specific sports such as baseball or golf.
Talk to an Orthopaedic Specialist
Of course, recovery from a shoulder replacement does not happen in a vacuum—nor should it. While this article provides a broad overview of the many factors that influence your recovery, perhaps the two most important factors are your individual health and your choice of orthopaedic surgeon. Only a discussion with a qualified orthopaedist can answer those questions.
Dr. Robert Rolf is a board-certified orthopaedic surgeon at Beacon Orthopaedics and Sports Medicine who provides extensive expertise in total shoulder replacements. Dr. Rolf can provide a comprehensive examination of your health and discuss what you can expect during recovery. For your convenience, Dr. Rolf meets with patients at Beacon’s Batesville, Lawrenceburg, or Northern Kentucky locations as well as Beacon West in Harrison, Ohio. Schedule an appointment online to meet with Dr. Rolf.
Tendon Injuries in the Shoulder FAQ
June 13, 2018
The shoulder is the most flexible joint in the human body. It consists of the three bones: the clavicle (collarbone), the scapula (shoulder blade), and the humerus (upper arm bone). It also consists of four joints: the glenohumeral joint, acromioclavicular joint, sternoclavicular joint, and scapulothoracic joint. These structures allow you to move your arm up and down, in front of you, toward the back, and in circles. This wouldn’t be possible, however, without powerful tendons and muscles.
The rotator cuff is a group of four muscles and tendons that help move and stabilize the shoulder joint. The rotator cuff muscles include the:
- Supraspinatus which assists in moving the arm away from the midline of the body.
- Infraspinatus which assists in the external rotation of the arm.
- Subscapularis which assists in the internal rotation of the arm.
- Teres Minor which assists in the external rotation of the arm.
These tendons and muscles in the shoulder are subject to frequent stress each and every day. Activities at home (e.g. cleaning, painting, and gardening), activities at the workplace (e.g. lifting boxes), and recreational activities (e.g. golf, tennis, and swimming) can all contribute to a shoulder tendon injury.
What are the common muscle and tendon injuries in the shoulder?
The most common muscle and tendon injuries in the shoulder include:
- Rotator Cuff Tendinitis
- Shoulder Bursitis
- Shoulder Impingement Syndrome
- Rotator Cuff Tears
While these conditions are closely related, there are key differences among them.
Rotator cuff tendonitis and shoulder bursitis are both forms of soft tissue inflammation caused by either direct shoulder trauma or—more commonly—minor, repetitive trauma. In fact, inflammation due to overuse is so common, especially among athletes, that it is also called tennis shoulder, pitcher’s shoulder, and swimmer’s shoulder.
Tendonitis refers to inflammation of shoulder tendons while bursitis is inflammation of bursae, or the fluid-filled sacs that act as cushions within joints. Symptoms include pain, stiffness, swelling, and limited range of motion.
Shoulder impingement syndrome occurs when rotator cuff tendons are pinched between the upper arm bone and the shoulder blade. Consequently, this can also cause tendons to become inflamed leading to tendonitis or bursitis. It’s important to note, however, that while impingement is likely to lead to soft tissue inflammation, it can also occur without it.
Rotator cuff tears are classified in several ways depending on their cause and severity. Rotator cuff tears can either be traumatic (resulting suddenly from an injury), chronic (resulting from overuse), or degenerative (resulting from age-related tissue weakening). Moreover, a tear is classified as either a partial thickness tear (an incomplete tear) or a full thickness tear (a complete tear where the tendon is separated from the bone).
Who is at risk of a shoulder injury?
There are several factors that increase an individual’s risk. These include:
- While younger patients are subject to shoulder injuries, older patients face a higher risk due to the degenerative weakening of soft tissue as well as years of wear and tear. Degenerative disorders tend to begin at age 40 and become increasingly more common as people age.
- Prolonged use of the shoulder can cause small tears in soft tissue to gradually increase in size. This is especially common in occupations (e.g. painting) and sports (e.g. baseball) that require repetitive overhead movements.
- Smoking decreases the flow of blood and oxygen to soft tissue in the body. This makes tissue more susceptible to injury and slows the healing process. It also makes it difficult to build muscle that can prevent future injury.
Despite these risk factors, shoulder injuries are not limited to a specific demographic—accidents can happen to anyone. Falling on an outstretched arm or receiving a direct impact to the shoulder will cause an injury. It is crucial that you consult an orthopaedist following these incidents.
How do you know you have tendonitis or bursitis?
Rotator cuff tendonitis and bursitis share similar signs and symptoms. These include:
- Pain and swelling in the front of your shoulder
- Pain from raising or lowering your arm
- Shoulder stiffness and redness
- Loss of mobility and strength in the affected arm
- Pain that interferes with sleep
Patients with tendonitis may also experience a “clicking” sensation within their joint.
How do you know you have impingement?
Signs and symptoms of shoulder impingement include:
- Sudden pain when lifting your arm
- Constant ache in your arm
- Shoulder or arm weakness
- Pain that interferes with sleep
How do you know you have a rotator cuff tear?
Signs and symptoms of a rotator cuff tear include:
- Pain and swelling in the front of your shoulder
- Pain that continues to increase over time
Do shoulder injuries heal on their own?
Mild to moderate cases of tendonitis and bursitis can heal on their own with a combination of rest, conservative treatments, and patience. Mild tendonitis requires approximately 6-8 weeks to heal. Moderate tendonitis may require up to 12 weeks.
Rotator cuff tears are more difficult to generalize. This is primarily due to the fact that tears vary greatly in size, from microscopic injuries to complete ruptures in which the tendon is completely torn from the bone. Moreover, there is the possibility that the first injury leads to a secondary tear. It is best to consult a shoulder specialist if you suspect a torn muscle or tendon.
How do you treat shoulder injuries?
First and foremost, take a break from activities that repetitively stress your shoulder. Also, stop any activity that causes your tendons to flare up. If your occupation or sport requires you to use your shoulder, modify your activities to reduce the strain on your tendons as much as possible. In most cases, you will need to make long-term adjustments in order to avoid recurrent injury.
The RICE (rest, elevation, compression, and elevation) method can also help reduce symptoms and expedite recovery. The RICE method includes:
- Applying ice or a cold pack to your shoulder for 20 minutes every 3 to 4 hours
- Compress your shoulder with an elastic bandage
- Elevate your shoulder above the level of your heart when sitting or lying down
While the majority of shoulder injuries improve with conservative treatments, more severe injuries such as full-thickness rotator cuff tears do not heal on their own. These injuries require professional treatment from a shoulder specialist.
When should you see a shoulder specialist?
A healthy shoulder is vital for a number of occupations and sports, let alone everyday living. Unfortunately, shoulder tendons and muscles are highly susceptible to injuries that cause pain and disability. Moreover, certain conditions can occur without obvious signs or symptoms. Early diagnosis and treatment are key to maintaining an active lifestyle.
Dr. Robert Rolf at Beacon Orthopaedics & Sports Medicine is available to answer all of your questions regarding muscle and tendon injuries in the shoulder. You can attend one of Dr. Rolf’s monthly, free Shoulder Talks at Beacon West. Visit his page for a list of upcoming dates. You can also schedule an appointment with Dr. Rolf for a complete evaluation of your shoulder.
FAQ Shoulder Fractures: Clavicle, Proximal, Humerus, Scapular
June 11, 2018
Any high-energy impact to the shoulder can cause a fracture in the bone; these types of impacts include falling, colliding with a wall, body-on-body collisions in sports, or acute trauma from a motor vehicle accident to name a few. Shoulder fractures commonly involve the clavicle (collar bone), the proximal humerus (top of the upper arm bone), or the scapula (shoulder blade). In this article, the shoulder experts at Beacon Orthopaedics will explore the different types of fractures, what to look for, and answer some of the most frequently asked questions we’ve heard from patients.
Dr. Robert Rolf of Beacon Orthopaedics and Sports Medicine has a passion for helping patients regain mobility, remove pain, and strengthen their joints to resume their favorite activities sooner. If you’ve recently discovered symptoms mirroring those illustrated in this article, schedule an appointment today to speak with Dr. Rolf about your options for treatment and recovery.
What are the different types of shoulder fractures?
Clavicle Fractures: Fractures along the long, thin bone that begins at the base of the neck and extends out to the shoulder—these can occur at any age as the result of a fall, a collision in contact sports, or a motor vehicle accident.
Proximal Humerus Fractures: Fractures along the top of the long bone that runs from the elbow to the shoulder—either at or just below the humeral head. These fractures can also occur at any age, but your risk increases with age and the onset of osteoporosis in the shoulder.
Scapula Fractures: Scapula fractures are rare, because a larger impact is required to fracture the scapula—the flat triangular bone located in your upper back. These shoulder fractures usually result from a bad collision in a contact sport or automobile accident. Patients who have sustained this type of fracture are more likely to also have sustained nerve injuries, rib fractures, or lung injuries.
What are the signs of a fractured shoulder?
General Findings, Signs and Symptoms of Shoulder Fractures:
- Sharp or aching pain
- Swelling and bruising
- Loss of range of motion in shoulder
- A grinding sensation when the shoulder is moved
- Discoloration on the skin and/or hematoma
Clavicle Fracture Findings:
- Bruising and discoloration
- Swelling around the middle or along the collarbone area
- An area along the collarbone area that may reveal a bump (the prominent ends of the fracture under the skin)
- Shoulder range of motion is limited, but not completely lost
Proximal Humerus Fracture Findings:
- Severe swelling around the shoulder
- Very limited movement of the shoulder
- Severe pain during shoulder movement
Scapular Fracture Findings:
- Pain during shoulder movement
- Severe swelling and bruising around the back of the shoulder
- Scrapes around the affected area
What do you do to treat a shoulder fracture?
Treatment Options
Non-displaced fractures require a sling to immobilize your shoulder until the fracture is stable enough to regain full mobility. If your arm is moved too much too early, this will not only delay the healing process, but it will result in residual stiffness in your arm, further loss of mobility, and running the risk of dislodging the fracture fragments further.
If your shoulder fracture has a large percentage of displaced bone fragments, surgical procedures may be necessary. Surgery could entail anything from reforming the bone using wires or pins or a plate that will reconnect the displaced bones to total shoulder joint replacement.
How to Know You Need Surgery
- Have you sustained a compound fracture that has broken the bone so it pierces your skin?
- Has your fracture severely displaced bone fragments within the affected area?
- Has your fractured caused a misalignment in your shoulder socket?
- Have you fractured more than one shoulder bone?
If you have answered yes to any of the above questions, schedule an appointment immediately to get a consultation.
How long does it take for a shoulder fracture or break take to heal?
If the shoulder injury was not severe, there is fairly rapid improvement and return of function after the first 4 to 6 weeks.
After a more severe fracture, your quality of life can be greatly affected for months, depending on your participation in the recovery plan set for you by your physician. Most shoulder injuries whether treated surgically or non-surgically will require a period of immobilization followed by rehabilitation of the joint. If you don’t comply to the guidelines, you risk bone fragment displacement and an elongated recovery timeline (or risk the need for surgery).
Your Rehabilitation Plan Could Include:
- Range of Motion Exercises
- Strength Exercises
- Manual Therapy
- Modalities
- Functional Training
Schedule a Consultation with a Shoulder Specialist
If you are experiencing any of the symptoms discussed in this article, schedule an appointment today and Dr. Rolf of Beacon Orthopaedics and Sports Medicine will work with you to create a detailed treatment plan to get you back to the activities you love most.
The Most Common Shoulder Injuries and How They’re Treated
June 5, 2018
The anatomical structures of the shoulder are all highly interconnected. So much, in fact, that shoulder injuries rarely affect just one area of the joint. A single shoulder injury can affect multiple muscles, ligaments, cartilage areas, tendons, and bones.
Unfortunately, injuries are most likely to occur in those who rely on their shoulder the most—over-head athletes. Shoulder injuries are exceedingly common among athletes, especially those who compete in baseball, swimming, tennis, and football. This is often due to the repetitive workouts and intense competition that high-performance athletes endure.
Shoulder injuries, of course, are not limited to athletes. Professionals who frequently use their shoulder—such as those involved in painting, yard care, or construction—experience a higher risk of injury as well.
No matter how a shoulder injury occurs, everyone wants the same result: a fast recovery.
Dr. Robert Rolf is a leading, board-certified shoulder specialist at Beacon Orthopaedics & Sports Medicine. He has helped hundreds of patients in the Greater Cincinnati region achieve lasting improvements following their injuries.
The following information provides information from Dr. Rolf about the most common shoulder injuries and how they’re treated.
Shoulder Anatomy

The shoulder is the most mobile joint in the body. It consists of three bones: the humerus, scapula, and clavicle. It also consists of many muscles and tendons that hold the shoulder bones in place and stabilize the arm through its full range of motion. The four major muscles and tendons of the shoulder come together to form the rotator cuff.
Here is an image to better illustrate the anatomical structure of the shoulder:
Rotator Cuff Tears
A rotator cuff tear occurs when any tendon of the rotator cuff rips, either partially or completely. Rotator cuff tears are among the most common types of shoulder injuries.
Rotator cuff tears are most common in people who repeatedly perform overhead motions. These tend to be people with active jobs—such as construction workers—or athletes, though anybody can end up with a rotator cuff tear whether they’re active or not.
Rotator cuff tears vary in severity from partial- to full-thickness tears, with partial tears being far more common. It’s possible for a patient to have a partial-thickness rotator cuff tear without even realizing it.
Symptoms of Rotator Cuff Tears
- Pain that radiates from the upper shoulder down the elbow
- Difficulty moving the afflicted shoulder
- Pain that becomes worse after laying on the afflicted shoulder
- A dully, achy sensation in the shoulder and upper arm
- Weakness when moving the shoulder
- Pain when raising arm overhead
Common Causes of Rotator Cuff Tears
- Acute trauma (such as a fall)
- Repeated stress
- Normal wear and tear (as the rotator cuff naturally becomes more brittle with age)
Treatment Options
Nonsurgical
- Exercise and rehabilitation overseen by a physical therapist
- Improving posture and shoulder biomechanics
- Corticosteroid injections
- Platelet injections
Surgical
There are two main surgical options for rotator cuff tear repair: tendon reattachment or partial-tear trimming (also called “debridement”). If the tear is full, the surgeon will reattach the torn ligament back onto the bone detached from. If the tear is partial, the surgeon will shave away the torn/frayed part of the rotator cuff, as that portion often causes the patient’s pain. Debridement only removes the damaged tissue and does not affect the stability of the rotator cuff.
In either case, the procedures are performed by shoulder arthroscopy. This is a minimally invasive surgical procedure that uses a small camera (called an arthroscope) to aid in examining and repairing the torn tendons without having to make a large incision or open the shoulder.
Shoulder Impingement
Shoulder impingement occurs when one or more rotator cuff tendons get trapped and pinched between shoulder bones during arm movement, causing extreme pain and swelling/inflammation of the rotator cuff.
Shoulder impingement is most common in people who participate in physical activities requiring repeated overhead movements—again, mostly athletes. Swimmers, softball players, basketball players, tennis players, and golfers are all high risk for impingement. In fact, shoulder impingement is so common in swimmers that it has the nickname “swimmer’s shoulder.”
Symptoms of Shoulder Impingement:
- Weakness of the shoulders
- Difficulty raising arms or reaching up behind back
- Shoulder joint pain that gets worse after overhead movement or sleep
- Pinching feeling when moving the shoulder
Causes of Shoulder Impingement:
- Any injury (such as a sudden fall) that causes the shoulder to swell
- Bone growth/abnormalities in the shoulder
- Shoulder osteoarthritis
- Overuse of the shoulder muscles
- Improper form when swimming
Treatments
Nonsurgical
- Steroid injections
- Daily stretching
- Cortisone injections
- Therapy and activity modifications
Surgical
Note: Surgery is typically only considered when several months of sport-appropriate nonsurgical rehabilitation efforts have failed.
Most shoulder impingement surgeries involve either shaving down part of the acromion in order to relieve pressure from the pinched tendons, or shaving off any bone spurs to achieve the same effect.
Dr. Rolf is able to perform the procedure using an arthroscopic technique, which means that there will only be two small incisions made into the shoulder; this will lead to less scarring and quicker healing.
Other Common Shoulder Conditions
What Does Physical Therapy for Shoulder Injuries Entail?
In the majority of instances, an orthopaedist will recommend physical therapy as part of the patient’s treatment plan.
Education
First, the therapist will educate the patient on how the shoulder functions. The goal of this step is to help the patient understand how their posture and biomechanics may have contributed to their injury, and also to teach them how to avoid those issues in the future.
Evaluating and Retraining Movements
For athletes, it’s likely that some sort of improper form contributed to their injury. So, in physical therapy, the therapist and doctor will identify the improper form (if there is any) and train the patient on how to adjust their body mechanics.
Manual Therapy
Manual therapy is when a therapist or doctor will move and massage the recovering body part, as opposed to the patient moving it themselves. This gets the shoulder moving, which increases blood flow to the area, helps reduce inflammation, facilitates healing, and helps to improve range of motion after surgery.
Strength Exercises
Strength exercises are performed in order to restore strength to the shoulder. The type of strength exercises depends on the specific injury. Some injuries are exacerbated by weak muscles that cause other muscles to compensate. The physician will identify any weak shoulder muscles and recommend exercises to strengthen those muscles. Some of these exercises will be performed in the presence of the physician while others can be performed at home.
Range-of-Motion Exercises
When the shoulder is painful, many patients naturally avoid using their arm. While this can help reduce the frequency of pain, it can also cause the shoulder to become stiff. Range-of-motion exercises are performed in order to restore flexibility in the shoulder.
Functional Training
The therapist will also teach the patient how to adjust their functional activities in order to accommodate their repaired shoulder. This may include how to swim, how to throw a ball, or how to place items on a shelf. These adjustments allow the patient to maintain their active lifestyle while lowering their risk of further injury.
Receive Personalized Advice from Dr. Rolf
While rotator cuff tears and impingement are among the most common shoulder injuries, shoulder pain can be caused by a number of conditions. Only a certified orthopedic specialist can accurately diagnose your condition and prescribe treatment that is appropriate for your specific injury.
Dr. Robert Rolf is a board certified orthopedic surgeon at Beacon Orthopaedics and Sports Medicine who provides extensive expertise in rotator cuff tears as well as other conditions related to the shoulder.
For your convenience, Dr. Rolf meets with patients at Beacon’s Batesville, Lawrenceburg, or Northern Kentucky locations as well as Beacon West in Harrison, Ohio. Schedule an appointment online to meet with Dr. Rolf to start your journey toward shoulder relief.
A Practical Guide to Common Shoulder Pains
June 5, 2018
There’s no shortage of shoulder pain going around. In fact, in 2006, an astonishing 7.5 million people went to the doctor complaining of shoulder issues, according to OrthoInfo.
It’s no wonder, since the shoulder is an essential part of everyday life no matter what you do. While athletes rely on their shoulders extensively, individuals with semi-active hobbies such as cooking or gardening also depend on healthy shoulders. This is why shoulder experts such as Dr. Robert Rolf—a board-certified orthopaedic surgeon with a specialty in sports medicine—are in such high demand at Beacon Orthopaedics and Sports Medicine. Without healthy shoulders, completing even just simple tasks can be a real struggle.
The shoulder is the only part of the human body that allows full 360º motion, although the hips come close. This extreme mobility requires a complex system of bones, cartilage, muscles, and tendons to seamlessly work together. And, similar to machines, the more moving parts there are, the easier it is for something to go wrong.
This article provides a practical guide to common shoulder pains and issues with treatment information provided by Dr. Rolf.
Pinching When You Raise Your Arm
What Does This Pain Mean?
If you feel a pinching sensation when you lift your arm above shoulder level, it’s likely that you have a shoulder impingement. When you raise your shoulder, the space between the acromion (shoulder blade) and rotator cuff becomes narrow. It’s possible for the acromion to rub against the tendons and bursae of the rotator cuff, causing pain. This rubbing or pinching is also called “impinging,” hence the name.
What Causes an Impingement?
Shoulder impingement has two main causes:
1. Pinching that results from swelling of the nearby muscles or bursae
2. Bone growths/spurs that press on the tendons
In either case, the decreased amount of space in the shoulder joint increases the likelihood that tendons will get pinched. Swimmers and over-head athletes (baseball, softball, tennis) are especially at risk for impingement because of how frequently they perform overhead motions.
What Are Your Treatment Options?
In some cases, the fix for impingement is simply to stop overworking the shoulder. If rest isn’t enough to reduce swelling, anti-inflammatory injections can be administered to the afflicted shoulder.
If nonsurgical treatments don’t relieve pain, surgery may be considered. Depending on the cause of the impingement, the surgeon will go into the shoulder and either removed the inflamed part of the bursa, remove part of the acromion (in a process called anterior acromioplasty) or shave off any bone spurs.
Inability to Move Your Shoulder Without Pain/Stiffness
What Does This Pain Mean?
These symptoms strongly suggest a condition known as frozen shoulder, which is also called adhesive capsulitis. Frozen shoulder is a long-term condition where the capsule of connective tissue that encloses your shoulder joint becomes stiff and tight. This makes it difficult to move your shoulder without extreme stiffness or pain. The condition can sometimes last for years.
What Causes Frozen Shoulder?
There is no conclusive answer to what causes connective tissue around the shoulder to grow tight and stiff; however, diabetes and reduced shoulder movements for long periods of time (like when recovering from an injury) have been shown to greatly increase the risk of developing frozen shoulder.
What Are Your Treatment Options?
Though surgical treatments for frozen shoulder exist, nonsurgical treatments are much more common (and often extremely effective). A combination of anti-inflammatory medicine and physical therapy often completely restore the shoulder back to a healthy state.
If nonsurgical treatment does not help, surgery can be performed that will cut, tear, and stretch the stiff shoulder tissue. These methods often relieve stiffness and pain once recovery is complete.
Pain and Tenderness when Your Shoulder is Touched
What Does This Pain Mean?
This pain suggests bursitis, which is inflammation of a bursa, a tiny fluid-filled sac that reduces friction between moving parts of the body. There are several bursae in the shoulder, but the one most commonly responsible for shoulder bursitis is located just below the acromion and is called the subacromial bursa.
What Causes Bursitis?
There are three main causes of bursitis. In order from most to least common, causes are, sudden trauma, overuse, and infection.
Sudden trauma, such as falling and landing on one’s shoulder, is by far the most common cause of shoulder bursitis. The trauma causes the bursa to swell with blood, which puts pressure on other parts of the shoulder and makes it tender to the touch.
If overuse is the culprit, bursitis often accompanies impingement or tendonitis of the surrounding area. Overuse is most common in people who frequently move with their arms over their head. This covers most athletes, but also includes many manual laborers such as painters or construction workers.
Infections are uncommon but can still cause bursitis. Infection is most common in those with a weak immune system, such as those with AIDS or cancer.
What Are Your Treatment Options?
The most effective treatment for shoulder bursitis depends on the cause, but rest and anti-inflammatory medicine are effective treatments. If necessary, corticosteroids can be injected into the shoulder to decrease swelling, or a surgeon can drain excess fluid from the bursa.
Physical therapy is less common for bursitis than other shoulder conditions, but it still helps speed along recovery in certain patients.
Pain and Weakness after Lying on the Affected Shoulder
What Does This Pain Mean?
This pain points toward a rotator cuff tear. A rotator cuff tear is when one or more tendons in the rotator cuff tear. There are two kinds of rotator cuff tears: full and partial thickness.
To visualize the differences between the two types of tears, it’s easiest to imagine a taut rubber band. A full-thickness tear is like a taut rubber band that has been cut. It no longer has any tension in it, and it cannot hold two things together any longer. A partial-thickness tear is like a taut rubber band that has a rip. It is still taut, but more pressure is on the part of the rubber band that is still attached, and it is more likely to rip in the future.
What Causes Rotator Cuff Tears?
Just as there are two types of rotator cuff tears, there are two main causes of rotator cuff tears: acute injury and degradation.
To keep with the rubber band metaphor, an acute injury is when too much force is put on a rubber band and it snaps. A degenerative injury is when a rubber band that has been pulled taut for a long time becomes more and more brittle until it eventually wears out.
In either case, repeated overhead activities put one at greater risk for a rotator cuff tear.
What Are Your Treatment Options?
Roughly 80% of rotator cuff tears respond well to nonsurgical treatment, according to OrthoInfo. This treatment often involves rest, activity modification (such as avoiding the motion that caused the injury), strength exercises paired with physical therapy, and steroid injections if needed.
However, nonsurgical treatments don’t actually repair the torn tendon, which is a problem since rotator cuff tendons heal very slowly. In some cases, surgery is the better option.
In rotator cuff surgery, the doctor reattaches the torn tendon to the head of the humerus.
When It’s Time to See the Doctor
Ideally, you should see an orthopaedist as soon as you suspect you have a shoulder injury; however, once your shoulder pain begins to affect your everyday life, it’s imperative that you see a physician.
These guidelines above are an excellent way to self-diagnose any shoulder issues you might have. However, this is not a substitute for professional medical advice. If you experience any of the aforementioned symptoms, it’s unlikely that your condition will improve until you consult a specialist.
Schedule an appointment with Dr. Rolf at Beacon Orthopaedics and Sports Medicine for a professional evaluation of your shoulder. Dr. Rolf has had world-class training in complex shoulder reconstructive processes and can help you feel better, faster.
Exercises to Prevent Shoulder Injuries in Athletes
June 1, 2018
The shoulder is indisputably the most complex joint in the body. The arm would be drastically less useful without the range of motion the shoulder provides. Unfortunately, the shoulder’s complexity also means there are countless complications that can impair its function.
Consider this: the shoulder “[was] responsible for sending 7.5 million people to the doctor in 2006,” according to the American Academy of Orthopaedic Surgeons. Of those, 4.1 million cases were related to the rotator cuff, the “cuff” of muscles that keep the shoulder in place and assist with its mobility.
It’s difficult enough to complete everyday activities with an injured shoulder, but when you are an athlete, your shoulder is as much a tool of the trade as a paintbrush to a painter or a hammer to a carpenter. And like any good tool, the shoulder needs maintenance and care to work properly.
This article describes exercises that will keep your shoulders strong and flexible. Perform these exercises 2-3 times a week in order to increase your strength and flexibility.
The Biomechanics of the Shoulder
The shoulder may be more accurately described as the “shoulder system,” as the shoulder itself is actually made up of multiple muscles, tendons, and bones. The group of muscles and tendons that stabilize the arm through its full range of motion is called the rotator cuff.
The four muscles and tendons that compose the rotator cuff are:
- Supraspinatus—abducts the arm
- Infraspinatus—laterally rotates the arm
- Teres Minor—laterally rotates the arm and provides stability
- Subscapularis—medially rotates the arm
Exercises to Prevent Shoulder Injury
Exercise #1: Internal and External Shoulder Rotation
Internal Rotation
This exercise is both strengthens the shoulder and increases its stability. Internal rotation isolates the subscapularis muscle.
To perform internal rotation, either put a towel in between your chest and armpit or tightly press your elbow against your side. Make sure your arm is bent at a 90º angle. While in that position, take hold of a resistance cable or exercise band and, without moving your elbow, bring your fist in towards your sternum. Be sure to maintain control over the band while you reset your arm into the starting position. Make sure all the power comes from your shoulder; do not move your hips or back at all during this exercise.
This is a gentle exercise, so if you feel any pain, stop immediately.
External Rotation
This exercise isolates the infraspinatus and teres minor muscles, and through strengthening and stretching them provides more stability to the shoulder.
External rotation is performed in exactly the same way as internal rotation, except that your hand should start in front of your scapula and rotate outward. To achieve this, you’ll either have to switch the band or turn 180º.
Exercise #2: Wall Shoulder Raises (Also Called Wall Angels or Wall Slides)
For non-athletes, this exercise helps to regulate neck posture, as it helps to fight against the trend of jutting out one’s neck that develops after a long time looking at computer screens. Wall raises strengthen all four rotator cuff muscles, and they also promote good biomechanics in general, which will lead to more fluid movement and increased flexibility.
To perform a wall raise, all you need to do is stand with your back against a wall and ensure that your head, elbows, and hands are all touching the wall. This exercise cannot be performed correctly unless the head, elbows, and hands remain touching the wall at all times. Once you are in position, simply raise your arms above your head and lower them back down. This will be easiest if you slightly arch your lower back. Repeat the exercise until tired.
Exercise #3: Lateral Arm Raise
Lateral arm raises are excellent for athletes because they isolate the supraspinatus muscle, which is responsible for stabilizing the shoulder joint when you raise your arm above your head. If the supraspinatus is injured, the resulting shoulder impingement is often debilitating for an athlete.
Unlike the other exercises mentioned, lateral arm raises are best performed with light dumbbells. To perform a lateral arm raise, hold dumbbells at your side and keep your arms straight without locking your elbows. Extend your arms straight out and over your shoulders. Once you get above your shoulders, your supraspinatus stops working and your deltoid and trap muscles take on most of the work. If you stop at the shoulders, the exercise is called a scaption.
Build Your Best Body with Beacon
The factors that determine your athletic performance are complex—just like your shoulder. Both depend on a number of factors working together working together in unison. If you would like to get your shoulder back into shape, schedule an appointment with Dr. Robert Rolf at Beacon Orthopaedics & Sports Medicine. Dr. Rolf and his team of certified physical therapists will work together to provide you with a personalized, comprehensive exercise plan to help you achieve your performance goals.
Total Shoulder Replacement or Reverse Shoulder Replacement
May 21, 2018
Shoulder arthroplasty, often called a total shoulder replacement, is a well-established surgery for treating severe pain and stiffness. In fact, approximately 53,000 people in the U.S. have shoulder replacement surgery each year in order to regain comfort and function, according to the Agency for Healthcare Research and Quality. And while the majority of these procedures would be considered standard replacements, patients may be surprised to know that a “reverse” replacement is also an option. In some situations, a reverse shoulder replacement may benefit a patient more than a standard procedure.
At Beacon Orthopaedics and Sports Medicine, our shoulder specialists have performed numerous total shoulder replacements and reverse shoulder replacements. If you are experiencing shoulder pain and stiffness that limits your activities during the day and keeps you awake at night, you should talk to a specialist about your options. Here is information about total shoulder replacements and reverse shoulder replacements to help guide your discussion.
Q: What is a total shoulder replacement?
In a healthy shoulder, the head of the upper arm bone (humerus) fits into a shallow socket in the scapula. In shoulder replacement surgery the damaged portions of the shoulder are removed and replaced with a smooth metal ball attached to a stem. This artificial component, called a prothesis, will either replace the “ball” of the joint or both the “ball” and “socket.”
Q: What is a reverse shoulder replacement?
 In reverse shoulder replacement surgery, the damaged portions of the shoulder are also replaced with a prosthesis made from metal and plastic. However, unlike a standard replacement, the artificial component is placed on the socket side of the joint. The socket is then placed on the arm side where it is supported by a metal stem. Thus, the prosthesis is reverse of where its natural counterparts would be located within the body.
In reverse shoulder replacement surgery, the damaged portions of the shoulder are also replaced with a prosthesis made from metal and plastic. However, unlike a standard replacement, the artificial component is placed on the socket side of the joint. The socket is then placed on the arm side where it is supported by a metal stem. Thus, the prosthesis is reverse of where its natural counterparts would be located within the body.
Reverse shoulder replacement works best for patients with cuff tear arthropathy or a detached rotator cuff. The reverse prosthesis allows the patient to use their deltoid muscles instead of their deteriorated or detached rotator cuff tendons in order to lift their arm. It is also effective in people with complex fractures or people who have extensive bone loss.
Q: What are the benefits of shoulder replacement surgery?
 First and foremost, the purpose of shoulder surgery is to relieve chronic pain and restore mobility so patients can resume normal living. Additionally, an orthopedic surgeon may recommend a shoulder replacement in order to treat the following conditions:
First and foremost, the purpose of shoulder surgery is to relieve chronic pain and restore mobility so patients can resume normal living. Additionally, an orthopedic surgeon may recommend a shoulder replacement in order to treat the following conditions:
- Osteoarthritis
- Rheumatoid Arthritis
- Post-traumatic arthritis
- Rotator Cuff Tear Arthropathy
- Avascular Necrosis
- Severe Fractures
- Bone Tumors
In recent years, advancements in prosthetic designs have allowed patients to resume active lifestyles following surgery. Patients can often return to baseball, golf, swimming, or many of the other activities they enjoy.
Q: How successful is shoulder replacement surgery?
Both total shoulder replacement and reverse shoulder replacement have been shown to be highly effective. As with all forms of surgery, however, the effectiveness of the procedure depends on the overall health of the patient, their participation in physical therapy, and the expertise of the orthopaedic surgeon. Patients can improve their outcomes by choosing an experienced orthopaedic surgeon and adhering to their treatment plan.
Q: What are the potential risks of shoulder surgery?
Shoulder replacements are considered as safe as hip and knee replacement surgeries. Of course, as with any joint replacement surgery, there are associated risks. The most common complication is the dislocation of the prosthesis, with dislocations being more likely to occur among reverse shoulder replacements. Fortunately, a dislocation can be managed by placing the arm back into the proper location and keeping the arm immobile for a period of time.
Shoulder replacement surgery also carries risks associated with other forms of surgery, including:
- Infection
- Fracture
- Nerve or blood vessel damage
- Joint stiffness or instability
- Loosening of the prothesis
- Dislocation
Although rare, other complications may occur. An experienced orthopaedic surgeon can talk to you about these complications and discuss your individual level of risk. In some instances, additional surgery may also be necessary.
Q: How long does it take to recover from shoulder surgery?
For the first 7-14 days following surgery, you will need someone to assist you with your daily activities at home as well as transportation. You should also expect your arm to be in a sling for the first 3-6 weeks and to participate in physical therapy for the first 8-12 weeks.
After about 6 weeks following your surgery, you may resume driving. At this time, you may also return to work depending on how much physical activity is required.
After 1-2 months you may resume lifting heavier objects above the shoulder level.
For most patients, shoulder surgery typically requires 3-6 months for a full recovery.
Q: Who is a candidate for shoulder replacement surgery?
The typical shoulder replacement patient is 50-80 years old. It’s important to note, however, that younger patients may also require surgery. Candidates for total shoulder replacements typically have debilitating, chronic pain or severely restricted joint mobility that interferes with daily activities. And while severe osteoarthritis, rheumatoid arthritis, or another form of the disease are common among patients, shoulder arthritis is not the only condition that may require surgery in order to treat.
Is Shoulder Replacement Appropriate for You?
Every patient’s situation is different and an experienced orthopaedic surgeon whether a total shoulder replacement or reverse shoulder replacement is appropriate for you. If you experience chronic pain and have not achieved relief with conservative, non-surgical treatments, contact Beacon Orthopaedics and Sports Medicine today to schedule an appointment with Dr. Rolf.
Frequently Asked Questions about Rotator Cuff Tears
May 21, 2018
Your rotator cuff is an integral part of your shoulder—helping stabilize the shoulder by holding the ball (humerus) and glenoid socket (scapula) together as you raise and rotate the arm. When the rotator cuff is torn and not functioning properly, shoulder weakness and pain is the result.
In this article, the Dr. Robert Rolf at Beacon Orthopaedics discussed common questions asked about the rotator cuff and rotator cuff tears.
How does the rotator cuff tear, and how do you know you’ve sustained a tear?
Rotator cuff tears can happen at any age, but are more common as we get older.
As you shoulder moves, the rotator cuff keeps the humeral head of the shoulder depressed into the glenoid socket. If the humeral head does not stay within the glenoid socket, it will elevate and hit underneath the acromion, the outside part of the scapula, and result in impingement. Impingement leads to bursitis (inflammation in the bursa) and tendinitis (inflammation in the tendon). This will ultimately result in partial then full-thickness rotator cuff tears. Clinically, people will start experiencing pain and weakness.
Athletes who play sports that require a lot of overhead activity are at a high risk for sustaining a rotator cuff tear. These tears can result from a single traumatic event—such as a sudden fall on your shoulder or a collision with an object or another player—or the tears can develop gradually because of repetitive overhead motions like pitching or throwing a ball.
One way to know that you’ve sustained a tear is through the following test:
- Sit yourself comfortably in a chair.
- Bend your elbow 90 degrees.
- Tuck your elbow into your side.
- Have someone push your hand in towards your belly as you try to push out.
If you are unable to hold that position and/or feel pain while trying to keep your arm in that position, you may have sustained a rotator cuff tear and should schedule an appointment to get a consultation.
What does it feel like to have a torn rotator cuff?
Common symptoms include:
- Vague pain in the front of your shoulder
- Pain that radiates down the side of your arm
- Recurrent pain with overhead activity
- Night pain that awakens you from sleep
- Weakness (especially when attempting to lift your arm)
- Loss of range of motion
- Difficulty raising the arm away from your side by yourself
- Catching or snapping sensation when you move your arm
Do rotator cuff tears heal on their own? How do you fix a rotator cuff tear?
Many times, rotator cuff tears can be treated with conservative methods such as anti-inflammatory medication, steroid injections, and physical therapy. If the tear is complete, meaning that there are no longer any fibers attached to the bone, it is likely that your rotator cuff will not heal on its own—in these cases surgery is recommended.
Conservative treatments and surgical treatments alike are designed to restore strength, functionality, and mobility to the involved shoulder and relieve your shoulder pain. Your orthopedic surgeon will help you decide the best plan of action for your shoulder.
What is the average recovery time for rotator cuff injuries?
In majority of the recovery can take 4 to 6 months or longer, depending on the size of the tear. Most activities can be resumed at 6 months, however the rotator cuff will heal for up to a year.
How important is rehabilitation in the treatment of a rotator cuff tear?
Rehabilitation plays a critical role in recovery—no matter if you are choosing nonsurgical or surgical treatment options. Proper rehabilitation to strengthen your rotator cuff muscles and your periscapular muscles will decrease her overall recovery time and help you reach your maximum function.
If surgery is the best solution for your tear, you may have to wear a sling for four to six weeks after surgery. Most people are involved in physical therapy for 3-6 months after surgery. Over time, you go to physical therapy less frequently, but continue to do a home based program.
Your orthopedic surgeon can talk through your options with you at length to discover the best program for you, based on your needs.
What positions should I rest my arm in after surgery?
Not all rotator cuff repairs are the same and a physician may modify your postoperative care based on what was done during surgery. Most repairs are placed in a sling with a pillow to wedge the arm away from the body and take some tension off the rotator cuff repair.
During the first stage of rehab, which may last up to 6 weeks, you will not be able to move your shoulder on your own. Your physical therapist we will move your shoulder for you and may even help you set up a pulley system at home to continue this passive motion. If you try to actively move your shoulder before the tendon is healed, you may disrupt the repair.
When resting, many people find it more comfortable to prop up in bed with a pillow behind the shoulder. Some people even prefer a recliner. Both of these options seem to be more comfortable than lying flat in bed.
Are there differences between an open and arthroscopic rotator cuff repair?
Arthroscopic repair is done through small portal incisions and is the most common way that rotator cuff tears are fixed. Some tears require a larger incision. While the incision sites look smaller with an arthroscopic procedure, it is important to remember that the same tissues were still repaired and thus the same postoperative precautions regarding tissue-healing time for repaired muscle/tendon are observed.
When to Talk to a Shoulder Specialist
If you’re concerned that you may have sustained a rotator cuff tear, and exhibit any of the symptoms listed in this article, or have been having difficulty moving your arm, schedule an appointment with Dr. Rolf.
Frequently Asked Questions about Shoulder Arthritis
May 21, 2018
Inflammation in your joints may be a result of degeneration called arthritis. This can cause symptoms ranging from pain, stiffness, loss of mobility to other consequences that can limit your lifestyle. Because your shoulder is comprised of three major bones (the humerus, scapula, and clavicle), inflammation results in discomfort and limited range of motion. In this article we will explore frequently asked questions about shoulder arthritis to help you get to the bottom of symptoms, treatment options, and concerns you might have.
What are the symptoms of shoulder arthritis?

-
- Pain:
- In the front, side or back of the shoulder
- While shoulder is in motion or staying still
- At night or in the morning
- While you sleep/after waking up
- While lifting or carrying heavy objects
- Worse after exercise
- Tenderness
- Redness
- Warmth in the joint
- Swelling and inflammation
- Loss of range of motion
- Grinding, clicking or cracking (crepitus)
- Shoulder joint locking up or sliding in certain positions
- Stiffness/Numbness
- Fatigue
- Fever
- Pain:
What are the different types of shoulder arthritis?
There are two joints in the shoulder, the acromioclavicular (AC) joint and the glenohumeral joint. Your shoulder can take a lot of wear and tear, but once your shoulder joint begins to show symptoms of pain, swelling and lowered mobility, there are higher chances that you are beginning to develop arthritis in the shoulder.
To provide you with effective treatment, your physician will need to determine which type of arthritis you have. There more common types of arthritis seen in the shoulder have been listed below.
Rheumatoid Arthritis (RA)
Patients who experience symptoms of rheumatoid arthritis—a chronic inflammatory disease of the joints that can cause erosion and deformation of your shoulder bones—are experiencing the consequences of their own immune system attacking their synovium (the thin membrane that lines your bones at the ends where they meet to create your joints).
There is symmetrical joint involvement in rheumatoid arthritis—if one shoulder is affected, your chances of experiencing symptoms in the corresponding joint on the other side of your body is high. This means you will not only have RA in one shoulder, hip, hand or knee, but you will likely have RA in both (or more). There are many other types of inflammatory arthritides. Most of them, including rheumatoid arthritis are treated with disease modifying medications to prevent your immune system from attacking the synovial lining of the joint.
Osteoarthritis (OA)
Osteoarthritis—a degenerative condition, also known as wear-and-tear arthritis, that destroys the smooth articular cartilage of the shoulder bones—is the most common type of arthritis in the shoulder and appears more common in the AC joint than in the glenohumeral joint, and is usually diagnosed in people over 50 years of age. The degenerative nature of OA leads to the rough bone ends in the shoulder rubbing against each other—resulting in irregular motion within the joint.
Osteophytes (bone spurs) play a big factor in the resulting irregular motion of the shoulder joint in OA, because when you combine the friction from the osteophytes that form as the bone tries to heal itself with the developing inflammation, your shoulder loses range of motion, and results in more pain and weakness as you try to move your arm. Many people will say that their motion has become “ratcheting”.
Other Joints OA Can Affect
- Hands
- Knees
- Hips
Post-Traumatic Arthritis
In the event of a shoulder injury, there is a chance you can develop arthritis in the shoulder joint—this type of arthritis is called post-traumatic arthritis (PA)—because shoulder injuries are commonly due to the shoulder joint’s instability, and the consequences of that instability. When you fracture or dislocate your shoulder joint, fluid can build up in your shoulder, causing pain and swelling and potentially leading to your shoulder developing PA. Trauma from sporting injuries and other accidents can also cause this condition.
How is arthritis diagnosed?
It’s important to find out what type arthritis you have because treatments vary for each type. Early diagnosis and treatment of arthritis is important to help slow or prevent further joint damage that can occur if you leave it untreated. But, to go a step further, it’s even more pertinent to gain clarity on which type of arthritis you have, and—because it sometimes takes a long time to clearly diagnose the type of arthritis you’re experiencing—it’s of critical importance to schedule your consultation as soon as possible if you believe you might have arthritis in the shoulder.
- Your doctor will examine the injured joint.
- What your physician is looking for:
- Pain level
- Range of motion
- Grinding severity
- Joint weakness
- Tenderness to touch
- Swelling and skin rashes
- Your doctor will also conduct some laboratory tests on the injured joint:
- Lab work is commonly performed when your physician is worried about an inflammatory arthritis. This may include bloodwork or joint fluid analysis.
- X-rays or advanced imaging such as MRI or CT scan
- What your physician is looking for:
- Loss of joint space
- Bone cysts and spurs
- Bone quality
- Bone wear
- Integrity of the soft tissue, mainly the rotator cuff
What are common arthritis treatments?
Once you’ve been diagnosed with arthritis, talk to your physician about the best treatment plan for you. Some patients see more benefits in recommended medications, but there are many things you can do to help manage pain and fatigue and regain some range of motion. Below is a list of some treatments you might discuss with your physician.
Medication
Many different medicines—both prescription and over-the-counter medicine—can treat arthritis. However, before you purchase or seek out any medication, you should always check with your doctor to be sure it’s ok to take them.
- Anti-inflammatories (NSAIDs)
- Aspirin
- Acetaminophen (Tylenol)
- Corticosteroids (injection or in pill form)
- Disease modifier medications (inflammatory arthropathies)
- Sleep medications
Exercise
Regular exercise is important to keep you moving—it helps lessen pain, reduce fatigue, increases range of motion and increases overall stamina. Be sure to exercise at a level that allows you to talk comfortably during the activity—and don’t be afraid to lower your level of impact and resistance to further reduce the amount of pressure on your shoulder. If you experience pain after exercising for more than two hours you may have done too much and need to take a rest.
Three types of exercises can help people with arthritis:
- Range of motion
- Strengthening
- Endurance
Heat and Cold Therapy
Applying hot or cold packs over joints and muscles help reduce inflammation and provide short-term relief from pain and stiffness. While using hot or cold packs to clear up some of your symptoms in the short-term, it’s important to use heat and cold safely in the long-term. Don’t use either treatment for more than 20 minutes at a time, because the longer exposure to drastic changes in temperature could damage your skin if you don’t let it return to normal temperature between applications.
Surgery
If nonsurgical treatments fail to relieve symptoms, your physician could recommend one of the below surgical treatments. When conservative measures fail, surgery can help reduce pain and increase movement in the shoulder.
Joint Replacement Surgery: Also called arthroplasty, this involves replacing the humeral head and the glenoid socket with an artificial prosthetic joint.
Arthroscopy: Arthroscopy is not as successful for glenohumeral arthritis. It is very successful for treating acromioclavicular joint osteoarthritis. Surgeon will use small incisions to clean out the shoulder joint—a tiny camera is inserted into the joint and this camera guides the surgeon to help remove the debris, and bone spurs.
Resection Arthroplasty: This is primarily for treating acromioclavicular joint osteoarthritis. It involves surgically removing 8-10 mm of the distal bone from your collarbone. In its place, scar tissue develops, decreasing the pain that resulted from the arthritic bone of the clavicle rubbing with the arthritic bone of the acromion.
Get a Consultation with Beacon and Say Goodbye to Your Arthritis
The inflammation from arthritis increases over time —leaving you with pain, fatigue, lack of mobility and constant frustration. While there is no cure for arthritis, especially arthritis in the shoulder, there are several treatment options available to you to help manage the pain and treat your symptoms like those noted above. If you are experiencing any of the symptoms discussed in this article, schedule an appointment today and Beacon Orthopaedics and Sports Medicine will work with you to create a detailed treatment plan to get you back to the activities you love most.
Shoulder Instability and Labral Tear FAQs
March 28, 2018

Because of the complex composition of the shoulder, you can position your arms and hands basically anywhere in space. But, for the very same reason, your shoulder is one of the easiest parts of your body to injure.
One of the most common of these injuries is shoulder instability or “shoulder looseness.” Since the shoulder is a ball and socket joint (where the top of your upper arm is the ball), an area of your body called the shoulder girdle is responsible for keeping the shoulder in place. It does this with the help of a round rim of fibrocartilage called the labrum and several ligaments. The labrum has the same effect on the shoulder as the rounded lip of a golf tee has to a golf ball. That is, the labrum helps the shoulder from slipping out of its joint. The ligaments also aid in keeping the shoulder stable and in joint.
When the labrum gets damaged or torn, it puts the shoulder at increased risk for looseness and dislocation. Two common ways this can happen are from sudden dislocation (often from a trauma such as falling on an outstretched arm) and repetitive strain (overuse injuries, etc). Both of these injury types lead to stretching and/or tearing of the labrum, causing joint weakness. This makes the labrum too loose to keep the shoulder in the socket while moving or adjusting into certain positions, creating overall instability of the shoulder. If one or more of the ligaments are torn, this can cause the loose or unstable feeling as well.
Frequently Asked Questions Regarding Shoulder Instability
Q: How will I know if my shoulder is loose?
Depending on the severity of the loose shoulder, you might not even notice it. Sometimes a loose shoulder only feels like a gentle popping when the shoulder is moved in certain ways, others feel their shoulder slide in and out of the joint at times. As looseness persists, you will find that you experience dull to severe pain when you try to move your shoulder. For athletes, particularly those who frequently use an overhead throwing motion (such as baseball pitchers), loose shoulders cause a decrease in power that is immediately noticeable. There is also a genetic condition called Ehler’s Danlos Syndrome that can cause loose or hypermobile joints. This is a connective tissue disorder that gives your joints increased elasticity.
Q: What is a shoulder labral tear?
The labrum is a pear-shaped bumper of cartilage that is attached to the shoulder socket rim, where the ball shaped humerus head fixes into the depression (glenoid) in the shoulder blade. This acts to keep your shoulder joint fixed and stabilized along with several ligaments.
Q: How do Shoulder Labral Tears occur?
The fraying and tearing of your labrum may be due to the wear and tear that comes naturally with age, or it could also result due to injury and/or stress to your shoulder. Other factors that contribute to shoulder labral tears include:
- Car Accidents
- Repetitive Overhead Activity
- Shoulder Dislocation
Labral tears can fall into any of the three following categories, based on the location of the tear. The categories are:
- SLAP Tears: A Superior Labrum from Anterior to Posterior (SLAP) tear is most commonly seen in overhead throwing athletes, and results from damages done to the top of the labrum.
- Bankart Tears: A Bankart tear occurs during a shoulder dislocation—when the shoulder comes out of joint, the labrum is torn, and the shoulder is more susceptible to future dislocations.
- Posterior Labral Tears: Posterior Labral tears occur when the rotator cuff and labrum are pinched together in the back of the shoulder.
Q: What are the symptoms of Labral Tears?
Symptoms of labral tears and shoulder instability include:
- Pain in the shoulder joint
- Unstable feeling during shoulder movement
- Locking and catching sensation in the shoulder joint
- Limited overhead activities
- Loss of shoulder strength and range of motion
- Loss of velocity when throwing
Q: How is a Labral Tear Diagnosed?
The best way to diagnose a labral tear is seeking an evaluation from an Orthopedic Physician. They will perform a clinical exam to evaluate for a tear. In order to do an evaluation, the Physician will perform several common orthopedic special tests that indicate a labral tear could be present. If the physician suspects a labral tear, further imaging is needed to confirm the diagnosis. Further imaging in the form of an MR arthrogram is typically ordered. The MR arthrogram is a little different than a typical MRI because dye is injected into the affected joint. This dye adds to the imaging test because the fluid from the dye can sneak under the tear and make it easier to detect on the images. This is the best way to interpret a labral tear short of having surgery.
Q: How is shoulder instability treated?
Instability can be treated with nonsurgical treatment (conservative) or surgically. Typically a course of conservative treatment will be tried before surgery is recommended. Nonsurgical treatments for shoulder instability can include:
- Lifestyle Changes
- Avoid the aggravation of current symptoms
- Anti-Inflammatory Medicine
- Cortisone Shots
- Physical Therapy
Q: What are some exercises I can do at home to help prevent shoulder instability?
First and foremost, shoulder instability is best prevented with resistance strength training—exercises that will help strengthen the muscles in your shoulder to maintain optimal joint stability. The OrthoInfo website is a good reference for information and exercises regarding instability.
Below are some of the exercises you can do to start improving your overall shoulder stability:
- Standing Rows
- External Rotations
- Internal Rotations
- Bent-Over Rows
Q: When is it Time to Consult an Orthopedic Physician?
If your shoulder pain persists despite at home treatment or conservative treatment from your Primary Care Physician, it is best to consult with an orthopedic surgeon to find out your options. Some of the potential surgical procedures to remedy labral tears are as follows:
- Labral Repair: this is an arthroscopic procedure that is used to either repair or debride the tear. A debridement involves removing frayed edges and any loose parts that get caught when your shoulder is moved—especially in smaller tears of the labrum. When your tear is large enough, suture anchors and heavy sutures are used to reattach the labrum to the socket. Doing this procedure arthroscopically helps minimize the incision size and cause less damage to the normal tissues surrounding the joint—leading to faster healing and recovery.
- Capsular Shift: this arthroscopic procedure is performed to tighten the joint capsule in the shoulder. In this procedure, your physician will tighten the capsule, and the ligaments that stabilize the shoulder together, in order to better stabilize movements in the shoulder joint.
- Latarjet Procedure: this open procedure is done when the shoulder socket experiences bone loss due to repeated dislocations. A small bone graft is taken from another part of the shoulder and placed into the worn away area of the shoulder socket. Once in the appropriate place, the bone graft is affixed to the worn area using screws to secure the graft in place.
Find Stability with Beacon Orthopaedics
If you’re concerned that you may have a labral tear or if your shoulder feels loose or unstable, contact us today to schedule an appointment.
Shoulder Pain and Snapping Scapula FAQs
February 16, 2018
Your shoulder is a complex machine, and your shoulder blade (scapula) plays a key role in its smooth operation. In fact, over a third of your shoulder’s movement depends on how well your scapula glides against your ribcage.
To help this gliding motion, your body has added a secret weapon: the scapulothoracic bursa. This tiny, fluid-filled sac acts as a cushion, reducing friction and ensuring pain-free movement as your shoulder blade slides back and forth.
So, what happens when that scapulothoracic bursa becomes inflamed from repetitive overuse or injury?
Dr. Robert Rolf, a board certified orthopedic surgeon at Beacon Orthopaedics and Sports Medicine, has compiled a collection of frequently asked questions about scapulothoracic bursitis, also known as Snapping Scapula Syndrome, below. In this article we’ll go over its cause, symptoms, and treatments.
If your question is not addressed in the collection below, Dr. Rolf offers free Shoulder Talks at Beacon West. If you’re interested in joining one of his shoulder talks, RSVP here and see when the next talk will be held.
What is Scapulothoracic Bursitis?
Scapulothoracic bursitis refers to inflammation in the bursa under the shoulder blade.
Also known as Snapping Scapula Syndrome, scapulothoracic bursitis occurs when the muscles underneath the scapula weaken and lead to a closer proximity between the scapula and the ribcage at rest and in motion. When the scapula cannot easily glide along the chest wall, the bones rub together. Over repetitive movements, the bursa becomes inflamed due to the constant friction.
What are the symptoms of Scapulothoracic Bursitis?
The following is a list of symptoms associated with a snapping scapula:
- Pain/aches in the shoulder area
- Grinding, grating and snapping sensation in the shoulder blade
- A potential lump from a bone growth on the scapula
- Tissue in the affected area often feels thick
- Swelling in the shoulder area
- Shoulder instability
- Tenderness or stiffness
What causes Snapping Scapula Syndrome?
Snapping scapula is caused by problems in the soft tissues—inflammation from repetitive movements—or bones of the scapula and chest wall. In some instances, the muscles under the scapula shrink (atrophy) from weakness or inactivity, leaving the scapula bone within a closer proximity to the rib cage. The resulting friction from bones bumping and rubbing together during movement causes the syndrome to develop.
Other potential causes are:
- Changes in the alignment or contour of the bones of the scapulothoracic joint
- Abnormal curves, bumps, or ledges on the upper edge of the scapula (called Luschka’s tubercles)
- Sustained, kyphotic (forward flexed) posture
- Inflammatory conditions such as rheumatoid arthritis
- Bone tumor such as an osteochondroma
- Poor Scapular Mobility
- Trauma or injury
How is Scapulothoracic Bursitis diagnosed?
A physical examination (where the shoulder and torso are completely exposed to ensure complete visibility) is performed on the affected area to begin diagnosis:
The patient is asked to raise and lower their arm for observation. The physician notes the range of motion and location of pain as the patient moves their arm.
In order to confirm diagnosis, your physician can potentially call for the following additional diagnostic tests:
- X-rays to view the shoulder joint’s bone structures in great detail.
- MRI scan to gain a better view of the shoulder’s soft structures and confirm the diagnosis.
What are the non-surgical treatment options for Scapulothoracic Bursitis?
In sports medicine, it’s best practice to always start with a conservative approach to treatment:
- Rest and ice the affected area
- Avoid direct pressure to the affected area
- Take anti-inflammatories to stop swelling
- Talk to your physician about a corticosteroid injection
- Do range-of-motion exercises every day to prevent stiffness
- Talk to your physician about a detailed physical therapy program
- Avoid smoking
What kinds of exercises can I do at home to help relieve my Scapulothoracic Bursitis symptoms?
To Enhance Range of Motion
Shoulder Pendulum Stretch
Use a 3-5 lb. object that you can easily hold with your affected arm. Bend at the waist so that arm holding the object is dangling straight down. (You may want to hold onto or lean against a table, chair, or wall with your opposing arm for support.) While keeping your dangling arm loose, gently rotate your arm in a circular motion while keeping your arm and shoulder relaxed. Rotate clockwise for 2-3 minutes and then counterclockwise for 2-3 minutes—repeating until your shoulder loosens up.
Internal Shoulder Rotation Stretch
Roll up one of your bath towels to create a long, thick “rope.” While, holding the towel at both ends—with the hand of your better arm positioned behind your neck, and the hand of the affected arm behind your lower back—pull your lower arm up by pulling up with your higher arm slowly. Once you’ve pulled your lower arm to where you feel resistance, hold the stretch for five seconds and then slowly return to the starting position.
Shoulder Flexion Stretch
With a non-weighted bar, stand up straight (core is tight, chest is up, and shoulder blades are back and down) holding the bar shoulder-width apart with your palms down. Then, keeping your arms perfectly straight, raise the bar up directly over your head, hold for 5 seconds and then slowly bring it all the way back down to the starting position.
Strengthening
Standing Scapular Elevation
Using reasonably weighted dumbbells (3-5 pounds), stand up straight (core is tight, chest is up, and shoulder blades are back and down) holding your weights loosely. Steady your grip on the weights and shrug your shoulders and traps straight up, keeping your arms straight as you lift. Hold this for five seconds and then slowly lower your shoulders back down to the starting position.
Upright External Shoulder Rotation
Using reasonably weighted dumbbell (3-5 pounds), stand with the dumbbell positioned out to the side of your head, elbow bent, and shoulder height with the dumbbell directly above the elbow. Slowly lower the dumbbell forward by rotating at the shoulder until the dumbbell is in line with your shoulder. Return the dumbbell the same way back to the starting position slowly.
What are the surgical treatment options for Scapulothoracic Bursitis?
If your condition hasn’t improved, and you are still experiencing symptoms of scapulothoracic bursitis, please schedule an appointment with Dr. Rolf at Beacon Orthopaedics to get your shoulder back in working condition.
In the event Dr. Rolf advises surgery as your best option, the procedure you can expect is usually performed arthroscopically—minimally invasive, with same day discharge, and a faster recovery.
Surgery may involve one or both of the following:
- Bursectomy: Removal of the inflamed bursa and any surrounding scar tissues or bone growth and other irregularities.
- Partial Scapular Resection: Removal of any bony prominences found on the scapula that may be rubbing on the rib cage.
What will my surgery recovery look like?
Following surgery your arm will most likely be immobilized in a sling for up to four weeks to allow the shoulder to heal.
Dr. Rolf, and the team at Beacon Orthopaedics, will then help you get on a detailed physical therapy plan to keep the shoulder moving well.
After approximately four weeks you will progress to active range of motion exercises and should be able to do most of your normal daily activities. Strengthening and resistance exercises are usually introduced after around twelve weeks. For most patients, full recovery is usually within 4 months post scapulothoracic bursitis surgery.
Know When You Need Surgery: Ask the Pros at Beacon
When it comes to surgery, the best physicians will recommend procedures only if non-surgical treatments failed to relieve you of your symptoms. You deserve more than a doctor, you deserve someone who is on your team, who has a team of professionals to ensure that your diagnosis is on point, your treatments are thorough, your recovery is detailed and you are given the support you need at every turn of the treatment plan.
Wellness is a journey. Let’s get you feeling better, together.
If you think you might be suffering from symptoms related to scapulothoracic bursitis, or have already tried non-surgical treatments for your constant shoulder pain to no relief, schedule your appointment with Dr. Rolf today.
Frequently Asked Questions: Suprascapular Nerve Entrapment
February 15, 2018
Suprascapular nerve entrapment is a rare condition that can be easily misdiagnosed or even go unnoticed by those who are affected. Let’s get to the bottom of this condition and talk about who could be affected, what body parts are involved, and what are the symptoms, causes and treatments of this potentially “silent” condition of the shoulder.
Dr. Robert Rolf, a board certified orthopaedic surgeon at Beacon Orthopaedics and Sports Medicine, has compiled a collection of frequently asked questions concerning suprascapular nerve entrapment below.
What is the suprascapular nerve?
Suprascapular nerve (SSN) is a sensory and motor (mixed) nerve that arises from the superior trunk of the brachial plexus with contributions primarily from the anterior primary rami of the C5 and C6 nerve roots, and supplies the supraspinatus and infraspinatus muscles. Both of these muscles are part of the rotator cuff muscle group—these muscles help perform and stabilize arm movements at the shoulder joint.
How can this nerve get injured?
- Trauma
- Vascular micro-trauma
- Irreparable related rotator cuff tears
- Fractures of the scapula (shoulder blade)
- Fractures to the clavicle (collar bone)
- Dislocation of the shoulder
- Gunshot/stab injuries to the shoulder
- Injury that results in stretching of the nerve
- Compression of the nerve caused by
- Tumors or ganglion cysts
- Thickened or calcified suprascapular ligament
- Congenital structural changes of the scapular bone
- SSN being fixed at two points (sling effect)
What is supracapular neuropathy?
Suprascapular neuropathy, or suprascapular nerve entrapment, is a condition which is due to irritation and damage to the suprascapular nerve (SSN). This condition can result in pain, weakness, or both depending on the cause. It is a relatively rare chronic condition that is commonly not diagnosed until other more common causes of shoulder pain have already been ruled out, such as:
- Rotator cuff tear
- Acromioclavicular joint disease
- Cervical spine (neck) disc disease
In fact, it often occurs that some patients end up getting surgery for the above conditions but recover and continue to have shoulder pain due to an unrecognized SSN irritation.
Is suprascapular neuropathy common?
Suprascapular neuropathy is generally believed to be a rare condition and probably accounts for less than 0.4% of shoulder diagnoses in patients with shoulder pain.
What are the signs and symptoms of suprascapular neuropathy?
The signs and symptoms of suprascapular neuropathy include:
- Shoulder/arm weakness or heaviness
- Radiating/burning pain to the neck, back or arm
- Pain that worsens with shoulder movement
- Loss of shoulder function
- Discomfort in shoulder and upper back
- Atrophy, wasting or shrinkage of upper shoulder muscles
- Denervation of the infraspinatus muscle
What causes suprascapular neuropathy?
The most common cause is the repetitive stretching of the SSN—generally due to consistent and exaggerated overhead movements of the shoulder. This is why the most common patients exhibiting symptoms of suprascapular neuropathy are athletes. Especially athletes who play baseball, volleyball, swimming, weightlifting and tennis (sports that require a lot of overhead activity).
However, other possible causes of this condition can include:
- Weak muscles controlling the scapula
- Falling on to the arm
- Broken scapula
- Torn rotator cuff
- Abnormal bone morphology of the scapular incisure
- Anomalies of the transverse ligament of the scapula
- Paralabral or ganglion cysts (nerve compression)
- Lesions due to traction
- Some surgical procedures like a Bankart Repair
What increases your risk of injury?
- Contact sports
- Football
- Rugby
- Lacrosse
- Poor strength and flexibility
- Repetitive overuse
How diagnosis for suprascapular neuropathy is found
Diagnosis for this condition remains largely a “diagnosis of exclusion”—where all other possible diagnoses are considered (and potentially treated) prior to this condition. This is, unless the physician remains alert to the diagnostic possibility of suprascapular neuropathy when the affected patient initially presents for consultation.
Tests that may prove helpful to confirm diagnosis:
- Electromyography/Nerve conduction study (EMG/NCV)
- Fluoroscopic x-ray
- Fluoroscopic ultrasound
- MRI
- Radiological study
- 3T Magnetic Resonance Neurography
What are the treatment options for suprascapular neuropathy?
Conservative Treatment Options
Physical Therapy
When the evidence of suprascapular neuropathy is confirmed but the conditions does not cause any pain or limitation of activity to the patient, then physical therapy exercises could be a possible solution provided by your physician. Exercises that encourage scapular/shoulder stabilization, mobilization, and flexibility could prove to be enough for relieving symptoms and resolve the condition, given proper time.
Pain Medication
If the patient experiences pain intense enough to want medication, nonsteroidal anti-inflammatory medications (such as aspirin and ibuprofen) or other minor pain relievers, such as acetaminophen, will often be recommended. Prescription pain relievers will only be given if deemed necessary by your physician.
Icing
Applying ice the affected area will relieve pain and reduce inflammation. As your physician will state, cold treatments should be applied for 10 to 15 minutes every 2 to 3 hours for inflammation and pain while at rest. For active patients, cold treatments are suggested to be applied immediately after any activity that aggravates your symptoms.
Heating
Heat treatments are most affective prior to the stretching and strengthening activities prescribed by your physician or physical therapist.
Surgical Treatment Options
If symptoms persist longer than 6 months despite conservative treatments listed above, then surgery may be recommended to the patient in order to release the entrapped nerve.
Arthroscopic decompression of the suprascapular nerve is a non-invasive surgical procedure in which the compressed nerve is released to relieve pain. Your physician will approach this surgery from the front (anterior) aspect of the shoulder, and access the nerve via a small incision on the top of the shoulder. Using the arthroscope, your physician will more easily view and decompress the nerve and have you out of the hospital and home ready to heal later that same day.
When should I seek medical care?
You should schedule an appointment with a physician if:
- Conservative treatment offers no benefit, or your symptoms get worse.
- Prescribed medications produce adverse side effects.
- Any complications from surgery occur:
- Pain, numbness, or coldness in the shoulder or arm.
- Discoloration of the nail beds (they become blue or gray) of the hands.
- Signs of infections (fever, pain, inflammation, redness, or persistent bleeding).
When You’re Not Sure, Consult a Shoulder Specialist
Suprascapular neuropathy is an uncommon condition. Because of its rarity, your symptoms might go unnoticed or be misdiagnosed. But, Dr. Rolf and the specialists at Beacon Orthopaedics won’t overlook any symptom without considering all the possible outcomes and causes.
Why do we focus on all of the details? Because when it comes to conditions such as suprascapular neuropathy, diagnosis can be a grey area. You need a physician who can be clear and confident in not only your diagnosis, but also your treatment plan.
If you think you might be experiencing symptoms of suprascapular neuropathy, schedule an appointment immediately. Dr. Rolf will talk through all of your symptoms and treatment options, and get you feeling better faster.
Frozen Shoulder FAQs
November 27, 2017
Frozen shoulder is a common, complex problem that affects many individuals. Despite ample research, a consensus over the true cause of frozen shoulder eludes us.
Dr. Robert Rolf, a board certified orthopaedic surgeon at Beacon Orthopaedics and Sports Medicine, has compiled a collection of frequently asked questions concerning frozen shoulder below.
The coming weeks will feature a collection of different FAQs about common shoulder conditions. This FAQ campaign is a digital extension of Dr. Rolf’s free Shoulder Talks that he hosts at Beacon West. If you’re interested in joining one of his shoulder talks, RSVP here and see when the next talk will be held.
In the meantime, let’s get to know a little more about the common questions about frozen shoulder.
Q: What is frozen shoulder?
A: Frozen shoulder is when your shoulder becomes gradually stiffer over time. Eventually, your range of motion decreases and this is often accompanied by extreme pain.
Q: How does frozen shoulder progress?
A: Frozen shoulder has three stages: freezing, frozen, and thawing. Freezing is when the shoulder’s range of motion gradually diminishes. Shoulder movement becomes progressively more painful during this stage. Pain tends to be worse at night. When the shoulder is frozen, range of motion remains limited, but pain may resolve. People with frozen shoulder regain full to near full range of motion during the thawing stage.
Q: How long does it take to go through the stages?
A: A very long time. For frozen shoulder to progress on its own through all three stages can take anywhere between 11 months to almost 4 years!
Q: How do you get frozen shoulder?
A: The exact cause of frozen shoulder is a mystery. The easiest way to develop it is to be in a position where you don’t move your arm for a long time, such as when you are recovering from an injury that requires you to keep your arm in a sling. Frozen shoulder can begin with or without antecedent trauma.
Q: Are certain demographics more likely to develop frozen shoulder than others?
A: Middle age women (40-60 years), diabetics, and those with thyroid diseases are at higher risk for developing frozen shoulder.
Q: What actually happens when a shoulder “freezes”?
A: The shoulder ligaments (the bands of muscle that hold the shoulder in place) become inflexible and stiff.
Q: How if frozen shoulder diagnosed?
A: Usually doctors can diagnose frozen shoulder by physical exam. X-rays or MRIs are also commonly used. It’s worth noting that frozen shoulder may present similarly to general inflammation of the shoulder joint or degenerative arthritis.
Q: How can I keep from getting frozen shoulder?
A: Avoid long periods of immobilization, unless it’s necessary, and make sure you’re always moving your shoulder. If you ever experience a reduction in shoulder range of motion and progressive worsening pain, see a doctor immediately.
Q: Can I get frozen shoulder twice?
A: It is possible, but it rarely occurs in the same shoulder. More often frozen shoulder develops in the opposite shoulder.
Q: After frozen shoulder, will my full range of motion be restored?
A: Most of the time, people who get frozen shoulder report that they get their full range of motion back.
Q: How is frozen shoulder treated?
A: Initially, frozen shoulder is treated with physical therapy and anti-inflammatory medicine (like ibuprofen). Steroid injections are useful at times. Surgery can be helpful when patients fail conservative treatment.
Q: Is frozen shoulder related to arthritis in any way?
A: Not necessarily, although some patients that have shoulder arthritis are often treated as if they have frozen shoulder.
Q: When is it Time to Consult a Shoulder Specialist?
If you are experiencing any extension of the symptoms mentioned above, or excessive shoulder pain. For more information or a clinical evaluation, please schedule an appointment with Dr. Rolf.
Preventing Shoulder Cuff Injuries in Athletes
July 7, 2017
The shoulder has the greatest range of motion of any joint in the body. It allows the arm to move away from the body’s midline, towards the body’s midline, forward, and backwards. It can also move the arm in a full circle, as well as rotate it towards or away from the midline. The articulation of the shoulder is so unique, in fact, that the hip is the only other joint in the human body that is also classified as a spheroidal joint, which is commonly known as a “ball and socket” joint.
While the rotator cuff is highly complex, it is also relatively weak. Similar to other structures of the body, it can be damaged by traumatic injuries, and is also extremely susceptible to wear and tear. Athletes who excessively use their shoulder—such as baseball and tennis players—are at the greatest risk of a rotator cuff injury. But, as any of these athletes would tell you, repetitive use of the shoulder is an unavoidable part of the game.
So what can athletes do to prevent rotator cuff injuries? Like all other sports-related injuries, prevention entails education, physical conditioning, and practice.
The Anatomy of the Rotator Cuff
The shoulder consists of the humerus (upper arm bone), the scapula (the shoulder blade), and the clavicle (the collar bone). The joint is formed from the spherical head of the humerus, which acts as a “ball”, and the glenoid cavity, which forms the “socket”.
The rotator cuff is a group of four muscles that come together at the head of the humerus. These muscles not only help stabilize the shoulder but they also keep the arm in its socket. In addition, each muscle also serves a specific, unique function related to movement.
- Infraspinatus: Rotates the arm laterally (away from the midline) at the shoulder joint.
- Supraspinatus: Helps the deltoid muscle abduct (raise) the arm at the shoulder joint.
- Subscapularis: Rotates the arm medially (towards the midline) at the shoulder joint.
- Teres minor: Rotates the arm laterally and weakly adducts (lowers) the arm at the shoulder joint.
Common Rotator Cuff Injuries
Rotator Cuff Tears
Rotator cuff tears are a common orthopaedic condition. When a rotator cuff muscle tears, it partially or completely detaches from the head of the humerus, causing shoulder pain and instability. Tears are most likely to occur in the supraspinatus muscle and tendon. Because these injuries result from a variety of causes and range in severity, they can be categorized in a number of ways.
Acute Tears
An acute tear results from a sudden injury, such as blunt force to the shoulder or a fall on an outstretched arm; however, a rotator cuff with pre-existing degeneration can also be torn by simple, everyday activities such as gardening or putting away the dishes.
Chronic Tears
A chronic tear, also called a degenerative tear, results from repetitive use of the shoulder cuff muscles over time. Athletes are at especially high risk for this type of overuse injury. Degradation, like the kind that is associated with chronic tears, occurs naturally with age as well. As such, people over 40 are at increased risk for this type of injury. Some common causes include:
- Reduced blood flow – Blood oxygen levels naturally decrease as people become older. Since oxygen is essential to all parts of the body, reduced oxygen both increases the risk of a rotator cuff tear and makes healing more difficult.
- Bone spurs – Bone spurs are little growths that occur on the bone as a result of too much calcium. These spurs rub on the rotator cuff, causing pain and degradation. Bone spurs can also lead to shoulder impingement, a condition where the arms cannot go above shoulder level without severe pain.
Signs of a rotator cuff tear include:
- A sudden tearing sensation
- Immediate weakness in your arm
- A cracking sensation when moving your arm
- Pain during certain movements
Symptoms of a rotator cuff tear include:
- Shoulder pain that gradually worsens over time and persists throughout the night
- Shoulder weakness that gradually worsens over time
- Difficulty performing overhead movements
A rotator cuff tear is described as either a partial or full thickness tear based on its severity.
Partial Rotator Cuff Tears
This form of injury is also referred to as partial thickness rotator cuff tear because the tear only extends part way through the tendon and often only involves one of the four rotator cuff muscles. It is more common than a complete tear and more common in younger individuals. And while seemingly less severe than a complete tear, there is no correlation between the size of a tear and the amount of pain it causes. In fact, in some instances, a partial tear can be more painful than a full-thickness tear.
Full-Thickness Rotator Cuff Tears
A full-thickness rotator cuff tear occurs when one or more muscles and tendons completely separate from the humerus. Large tears can cause significant shoulder weakness. For example, an individual may have to support their injured arm with their other arm when lifting or moving an object. Large tears can also cause a loss of shoulder mobility; however, this is not always the case.
Tendinitis and Bursitis
Tendinitis causes tendons to become swollen and painful, often due to over use and inflammation. Similarly, bursitis occurs when bursae—small fluid-filled sacs between bones, tendons, and muscles—become inflamed. These conditions can occur alone or simultaneously and are more likely to occur in people age 40 or older.
Tendonitis, in particular, is often a precursor to a tear. When tendons become inflamed, they scrape against the bones in the shoulder joint. This frays the tendons and consequently makes them more susceptible to tears.
Treatments for Rotator Cuff Injuries
First Aid
RICE (Rest, Ice, Compression, and Elevation) should be applied as soon as possible after an injury occurs. Rest provides time for the injury to heal while ice and compression reduce the amount the amount of swelling. In the case of rotator cuffs, however, individuals may forgo elevating the arm if it is difficult or uncomfortable.
Professional Treatment
The majority of rotator cuff injuries can be treated with a combination of rest and physical therapy. Physical therapy helps restore shoulder flexibility and strength as well as reduce pain.
If a patient does not achieve relief with conservative treatments, a physician may recommend orthobiologics, which is centered on the body’s own ability to itself. orthobiologics aids the body in creating new, functional tissue to replace old and damaged tissue.
Surgery is also an effective option; however, it is often a method of last resort. Candidates for surgery have symptoms that limit normal, everyday function and do not improve with conservative treatments. A talk with an orthopaedic specialist can determine if surgery is the right option for you.
How to Prevent Rotator Cuff Injuries
In general, the best way to prevent rotator cuff injuries is to strengthen the rotator cuff. Keep in mind that even simple, daily exercise can go far in strengthening muscles and tendons. The “doorway stretch” is one such exercise that can be performed at home. To perform the exercise:
- Stand in an open doorway and spread your arms out to your side.
- Grip the sides of the doorway at shoulder height.
- While maintaining your grip and keeping a straight back, lean forward until you feel a light stretch in the front of your shoulder.
- Slowly return to the original position. Repeat 10 times.
As always, speak with a physical therapist before starting an exercise program.
In addition to exercise, athletes should focus on proper form. Improper form puts increased stress on the rotator cuff and increases an athlete’s risk of an injury. Frequent breaks can help an athlete avoid fatigue that consequently leads to improper form.
When to See an Orthopaedic Specialist
While the majority of rotator cuff injuries heal with rest, it’s a slow process. Moreover, because many everyday activities require the use of the shoulder, patients can potentially worsen their condition by not seeking early treatment. For all of these reasons, it’s important to talk with an orthopaedic specialist at the first sign of an injury. An orthopaedist will ensure that you’re on the best path to recovery.
Dr. Robert Rolf is a board certified orthopaedic surgeon at Beacon Orthopaedics and Sports Medicine who provides extensive expertise in rotator cuff tears as well as other conditions related to the shoulder or elbow. Patients can meet with Dr. Rolf at Beacon’s Batesville, Lawrenceburg, or Northern Kentucky location as well as Beacon West in Harrison, Ohio. Dr. Rolf also offers informational Shoulder Talks at Beacon West. For a list of upcoming talks, visit Dr. Rolf’s page.
Frozen Shoulder: Symptoms, Causes and Treatment
June 8, 2017
The shoulder is one of the most complex joints of the body. In its most simplified form, it is made up of the humerus (bone in upper arm), scapula (shoulder blade), and clavicle (collarbone), as well as numerous muscles, ligaments, and tendons that provide the shoulder with its full range of motion. There are also several bursa throughout each shoulder. These fluid-filled sacs sit between bones, providing lubrication that allows for painless movement.
 This high level of complexity is what allows you to extend your arm forward and backwards; raise it upwards and lower it downwards; and rotate it in a circular motion. When the shoulder is healthy, these motions can be made with very little effort. Unfortunately, the shoulder’s intricacies also place it at greater risk of problems. Even a relatively minor injury that begins in one area of the shoulder can eventually make the whole region more difficult to use. In addition, movement will become much more limited and painful.
This high level of complexity is what allows you to extend your arm forward and backwards; raise it upwards and lower it downwards; and rotate it in a circular motion. When the shoulder is healthy, these motions can be made with very little effort. Unfortunately, the shoulder’s intricacies also place it at greater risk of problems. Even a relatively minor injury that begins in one area of the shoulder can eventually make the whole region more difficult to use. In addition, movement will become much more limited and painful.
Frozen shoulder, also known as adhesive capsulitis, is one such condition that begins mild and becomes worse if not treated early. However, unlike more well-known conditions–such as shoulder arthritis, impingement, and rotator cuff injuries—it is often not identified as the source of someone’s discomfort until symptoms have become more severe. This is why it’s important to know about the condition/recognize symptoms, so patients can see an orthopedic specialist for early treatment.
What are the Symptoms of Frozen Shoulder?
As the name implies, the hallmark sign of frozen shoulder is the inability to move the shoulder. It is primarily caused by the shoulder capsule thickening; however, stiff bands of tissue called adhesions can also contribute to the stiffness. Pain is also caused by a reduction in synovial fluid in the joint, which is meant to reduce friction during movement.
Symptoms of frozen shoulder typically develop slowly over a span of several months up to about two years. The development of symptoms can be classified into four stages: a pre-freezing stage, a freezing stage, a frozen stage, and a thawing stage.
The Pre-Freezing Stage (Months 1-3)
The shoulder will ache when not in use and develop a sharp pain with movement. Individuals will also notice a mild reduction in their ability to raise and rotate their arm, as well as reach behind their back.
While it may be difficult to distinguish the early signs of frozen shoulder from other, similar conditions, it is best to see any orthopedic specialist for any condition that lasts longer than two weeks. This is because most acute injuries resolve with rest, ice and immobilization within one-two weeks.
The Freezing Stage (Months 3-9)
Individuals will experience a progressive loss of shoulder movement. Scar tissue will also form and the bursae in the shoulder will become inflamed, causing increased pain.
The Frozen Stage (Months 9-14)
Individuals will experience a severely limited range of motion. At this point, the stiffness will make common tasks like cleaning or putting away groceries difficult. Severe pain will also persist during the early part of this stage but will likely decrease or go away entirely toward the end.
The Thawing Stage (Months 15-24)
The shoulder’s strength and range of motion gradually returns to normal.
What Causes Frozen Shoulder?
When a shoulder starts to freeze, some of the ligaments that connect muscles to bones are replaced by scar tissue. This scar tissue is not only brittle and inflexible, but it can also cause painful inflammation in the shoulder, especially the bursa.
It’s not known what causes a shoulder to freeze in the first place; however, there is clear data about who it is most likely to affect. Frozen shoulder occurs most frequently in women aged 40-60. It is also more prevalent in individuals who have diabetes, hyper- or hypothyroidism, cardiovascular disease, tuberculosis, or Parkinson’s disease. Individuals who are recovering from a shoulder injury are also at higher risk for frozen shoulder because an underused shoulder is more likely to freeze.
Treatments for Frozen Shoulder
Stretching and exercise can help manage the symptoms of frozen shoulder, no matter what stage a person is in. In fact, it’s highly recommended to both talk with a physician and begin regular stretching immediately after noticing the first signs of the condition. Stretching will not only strengthen the shoulder, but it will also help maintain mobility and reduce the buildup of scar tissue.
Finger Walk Exercise
- Face a wall and stand about an arm’s length away.
- Reach your arm straight out and touch the wall with your middle and pointer fingers only (it will be like you’re holding up a peace sign).
- With your elbow slightly bent, walk your fingers up the wall until you’ve gone up as far as you comfortably can. Your fingers should do all the work here. Also, make sure you stretch to the point of tension but not pain.
Exercise Band Inward Rotation
To do this exercise, all you need is a small resistance band and a door
- Stand next to the closed door and hook one end of the band around the doorknob.
- Hold the other end with your frozen shoulder arm and, while holding your elbow at a 90-degree angle, pull the band towards your body two or three inches and hold for five seconds.
- Repeat up to 15 times if you are able.
Talk to a Specialist
Frozen shoulder, like any loss of mobility, is scary. The good news, though, is that early treatment will dramatically reduce the onset of severe stiffness and pain.
If you are experiencing the signs of a frozen shoulder, you can turn to Dr. Robert Rolf at Beacon Orthopaedics and Sports Medicine. With world class expertise in orthopedic surgery and sports medicine, he is uniquely qualified to treat patients with frozen shoulder as well as a range of orthopedic conditions related to the shoulder or elbow.
You can schedule an appointment online to meet with Dr. Rolf at Beacon West in Ohio, Beacon’s Batesville or Lawrenceburg locations in Indiana, or Beacon’s Northern Kentucky location.
Total Shoulder Replacement: A Treatment for Shoulder Arthritis
April 17, 2017
Shoulder arthritis can be debilitating in many patients, resulting in persistent lateral arm pain that limits many activities of daily living, such as getting dressed, putting deodorant on or washing your hair. Many times, the pain of arthritis even awakens a person at night.
Osteoarthritis, which is sometimes called degenerative joint disease, and rheumatoid arthritis, a chronic disease that occurs when the body’s immune system attacks its own joints, are two of the primary forms of arthritis that affect the shoulder joint. Osteoarthritis and rheumatoid arthritis affect an estimated 31 million and 1.5 million Americans respectively, according to the Arthritis Foundation. This means that approximately 1 in 10 Americans will develop either of these diseases, if not another form of arthritis, that places the health of their shoulder at risk.
Due to advances in technology, including newer, more anatomic implants and improved perioperative pain control, total shoulder replacement offers an effective solution for individuals who suffer from shoulder arthritis and, consequently, shoulder pain.
Dr. Robert Rolf, a board-certified orthopedic surgeon and sports medicine specialist, performs many of the total shoulder replacements at Beacon Orthopaedics and Sports Medicine. In fact, Dr. Rolf is able to perform outpatient total shoulder replacements. This provides a cost efficient and time saving model for patients, allowing them to return home to recover instead of spending the night in a hospital.
Based on Dr. Rolf’s extensive experience in treating patients throughout the Greater Cincinnati area, here is information about total shoulder replacement and how to prepare for the operation.
What Is Total Shoulder Replacement?
![]()
Total shoulder replacement, also known as total shoulder arthroplasty, is a well-established and effective surgical treatment for joints that have been irreversibly damaged by arthritis or a degenerative disease.
A total shoulder replacement differs from a traditional replacement in a few key ways. First, the use of newer prosthetic designs allows patients to be more active than they have traditionally been, returning to sports such as golf, swimming, and tennis. Second, emerging trends in perioperative pain management allow the procedure to be performed in the outpatient setting, similar to patients who undergo rotator cuff surgery. This revolutionary approach to shoulder replacement not only allows the patient to return home quickly and recover in the comfort of their own home, but it also significantly reduces the cost of the procedure.
Candidates for Total Shoulder Replacement
While shoulder replacement is less common than knee or hip replacement, candidates for these surgeries share many similarities.
A suitable candidate for total shoulder replacement has chronic pain that prevents them from completing ordinary daily tasks. While this pain is often the result of severe osteoarthritis, rheumatoid arthritis, or another form of the disease, individuals who have had their shoulder joint irreversibly damaged or suffer from debilitating pain caused by another condition may also be suitable candidates.
Keep in mind that most patients should try more conservative treatments prior to considering surgery. Not every patient qualifies for a total joint replacement. Surgery is often reserved for individuals who have attempted conservative, non-surgical treatments for their condition with no success. The best way to determine if you are a suitable candidate is to schedule an appointment with Dr. Rolf or another orthopedic surgeon with fellowship training in shoulder surgery.
Preparing for Shoulder Surgery
If you’ve ever asked your family or friends about shoulder surgery, they likely went on about how it was the most painful surgery they ever experienced. They likely also said that it took nearly a year to recover, let alone return to sports, exercise or the other physical activities that they enjoy. Fortunately, there are steps you can take prior to your operation that will minimize your potential discomfort and help you achieve an optimal recovery.
Choose an Experienced Shoulder Surgeon
Without a doubt, the specialized training and expertise of your orthopedic surgeon will be a significant influence on your outcomes, if not the primary determiner. For this reason, it is paramount that you take the time to select an orthopedic specialist who you can place the greatest amount of confidence in, not just one who sees a large volume of patients.
Consider this: shoulder arthroscopy involves the use of saline to inflate the problematic joint so the surgeon has a better view while they work. The longer the surgery takes, the more swelling that will occur, consequently making the operation increasingly difficult. An experienced and efficient surgeon will not only keep the length of the surgery to a minimum, but also minimize the amount of swelling that may occur.
It is also important to know what to expect during the days, weeks, or even months following your procedure. One way to set a level of expectations for yourself is to ask your physician what steps they take to monitor their patients’ outcomes. A qualified physician will provide objective data on how their patients have improved since having shoulder surgery.
Choose an Experienced Physical Therapist
State-of-the-art preoperative pain management and patient-focused physical therapy can enhance your recovery. In fact, the physical therapist that you work with is perhaps the most critical component in your recovery.
Just like physicians, physical therapists can have specific areas of focus or have conditions that they treat more frequently than others. This is why at Beacon Orthopaedics, we provide physical therapy on site at several of our locations. If you opt to have surgery or therapy elsewhere, it is well worth your time to choose a physical therapist who understands exactly what you need following shoulder surgery. Moreover, finding a therapist that has a long-standing relationship with your physician is even better. This will ensure that your therapist has a complete understanding of how to go about your rehabilitation.
Practice Donning and Doffing
Sometimes, using the sling can be the most humbling part of the experience. Practice putting the sling on and removing it before surgery to limit your frustrations when you only have one good shoulder to put the sling on. This is particularly important for those who undergo surgery in an outpatient setting. After all, since these types of patients can expect to return home the same day of their operation, they should be self-sufficient enough to manage their sling.
Discuss Surgery Options with Dr. Rolf
Shoulder replacement surgery is technically demanding and, like all forms of surgery, should only be performed by a skilled, experienced, sub-specialty trained physician.
Dr. Robert Rolf is one of the fellowship-trained, experienced physicians that you can talk to about surgery at Beacon Orthopaedics and Sports Medicine. Not only is he board certified in Orthopedic Surgery, but he also has his Specialty Certificate in Sports Medicine.
In addition to world-class expertise in shoulder replacement, he can also discuss with you arthroscopic techniques for shoulder instability and rotator cuff tears or complex reconstructive procedures such as tendon transfers. You can schedule an appointment online to meet with Dr. Rolf at Beacon West in Ohio, Beacon’s Batesville or Lawrenceburg locations in Indiana, or Beacon’s Northern Kentucky location.
You can also attend one of his free Shoulder Talks to learn more about shoulder pain, treatment options, and related topics. For a list of dates and for RSVP information, please visit Dr. Rolf’s page.
UCL Injuries of the Elbow
March 23, 2017
What is the UCL?
The UCL (Ulnar Collateral Ligament) is a ligament on the inside part of the elbow. There are three bones that make up the elbow joint: Humerus, Ulna and Radius. The elbow joint is unique because it can bend and straighten as well as rotate and twist. There are two ligaments in the elbow that aid in preventing the elbow from dislocation-the RCL and the UCL. The UCL helps to connect the upper arm bone (Humerus) to one of the forearm bones (Ulna). The UCL stabilizes the elbow during the throwing motion, so it must be able to withstand a great amount of stress. There are also several nerves that run through the elbow and supply sensation to the forearm and fingers.
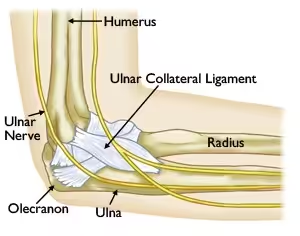
How do UCL injuries occur?
UCL injuries are very common for throwing athletes and those that use their upper extremity frequently. They can result from an acute injury (sudden onset) or from a chronic injury (over time). An acute injury can occur if too much stress is put on the elbow in one single incident which can cause the ligament to tear. An audible ‘pop’ typically can be heard or felt with this type of injury and intense pain may accompany this.
A chronic injury typically occurs from repeated stress on the ligament from throwing or swinging the arm over time. This causes the ligament to be stretched, frayed or torn. If the ligament is stretched, the repetitive motion of throwing can cause small micro tears in the ligament which can result in rupture of the ligament. Chronic injuries are more common than acute injuries for this ligament.
If there is an injury to the UCL it is often classified as a sprain. There are three grades of sprain: grade 1, 2 and 3. A grade 1 sprain means that the ligament is stretched but no tear is felt. A grade 2 sprain indicates the ligament is stretched and a partial tear could be present. A grade 3 sprain indicates there is a complete tear of the ligament.
What are the symptoms?
The most common symptom of a UCL injury is pain on the inside (medial) part of the elbow, especially during the acceleration phase of throwing. Swelling can also be present. If an acute injury occurred, swelling and bruising may also be noticed. A sensation of popping, grinding or clicking can sometimes be felt when throwing.
How are UCL injuries diagnosed?
If you notice any of the symptoms mentioned above, seeking an evaluation by a physician is the next step in diagnosing the injury. The physician will most likely do x-ray’s to rule out any type of fracture, stress reaction or loose fragments in the joint. During the physical exam portion, the physician will do several special tests to evaluate for a UCL injury. The most common test is called the Valgus stress test. A force is placed on the outside of the elbow which “opens up” the inside part of the elbow. If the UCL is working properly, it should stop the joint from opening up. If laxity (looseness) is felt during this test, it is indicative of a UCL sprain or tear. If laxity or pain are felt, this is indicative of a UCL sprain or tear. There are other special tests that can be performed, but the Valgus stress test is the most common.
If there is pain along the inside of the elbow and the Valgus stress test is positive, the physician will typically order an MR arthrogram. This is an MRI but dye is added through an injection into the elbow joint. The dye helps to make the test more accurate in that it goes into the space where a tear could be to make the tear easier to detect. If there is a tear present, surgery may be the best option to repair the tear.
How are UCL injuries treated?
UCL sprains can be treated conservatively or surgically. Conservative treatment includes rest, anti-inflammatories, physical therapy and bracing. Initially, rest and anti-inflammatories can be used to help reduce the pain and swelling. If the injury is acute, a sling may also be useful to aid in resting the elbow. Physical Therapy is a great resource for UCL injuries because it helps strengthen the muscles surrounding the elbow. This makes the elbow stronger and in turn helps to decrease the chance for further injury. A Physical Therapist can also evaluate the throwing mechanics to see if any changes need to be made in order to reduce the amount of stress on the elbow. Bracing can also be considered for support of the elbow or to reduce the amount of motion the elbow can have.
If there is a complete tear of the ligament or if pain and dysfunction persists despite conservative treatment, surgical intervention may be considered. This would include repairing the tear or reconstructing the tear. Many people are familiar with the name of this surgery which is called Tommy John’s surgery. The name is coined from the first person to ever have this type of surgery. This repair is performed when the ligament has completely torn off the bone. This is done by making an incision on the inside part of the elbow and reattaching the ligament to the bone. Sutures are used to keep the ligament in place when reattached to the bone. A reconstruction is performed when the ligament is unable to be reattached to the bone. A ligament in your wrist, called the Palmaris Longus, is often used to replace the UCL ligament if a reconstruction is performed.
What is the recovery after surgery?
Most patients are typically put in an elbow brace that limits range of motion after surgery. Each physician has different parameters for working on range of motion after surgery, but Physical Therapy will be required. The focus of Physical Therapy will be to get the proper range of motion back after surgery, although some patients may notice they have less range of motion than before. After this is achieved, the main focus will be strengthening the muscles surrounding the elbow and getting the person back to functional activity.
What’s the take away message?
Injuries to the UCL of the elbow are common, especially among throwing athletes and those who have to use their upper extremities for their sporting activity. If you notice pain along the inside of your elbow, you should seek treatment from an Athletic Trainer, Physician Assistant, Primary Care Physician or Orthopedic Surgeon. These healthcare providers all can evaluate the injury and formulate a treatment plan to help you get back to your sport.
Shoulder Labral Tears
March 21, 2017
Shoulder labral tears are a common acute injury. Learn more about how tears occur and some of the best options to fix them.
What is the Labrum?
Let’s start simple: The shoulder joint is comprised of 3 major bones: wing bone (scapula), collarbone (clavicle) and upper arm bone (Humerus). The Labrum surrounds the shoulder socket (Glenoid). The Glenoid Labrum is a bumper of cartilage that surrounds the shoulder joint and is pear-shaped. The purpose of the Labrum is to help stabilize the shoulder joint and keep the Humerus in the socket.

How do tears occur?
Labral tears can occur from an acute injury (sudden onset) or chronic injury (occurs over time). Acute injuries commonly occur from a fall on the shoulder when the arm is outstretched, lifting something heavy, or taking a blow to the shoulder. Chronic injuries often develop in a throwing athlete or a person that does repetitive overhead motion for their job. Oftentimes when a person dislocates (pops out of joint) their shoulder, a Labral tear results from the injury.
What are the types of tears?
There are several different types of Labral tears that can occur. These include SLAP tears, anterior tears, posterior tears and Bankart tears. SLAP tear stands for “Superior Labrum Anterior Posterior” which means that the tear is in the upper part of the labrum and extends to the back and the front of the Labrum. An anterior tear means that the front part of the Labrum is torn and a posterior tear means that the back portion of the Labrum is torn. Bankart tears usually result when a person dislocates their shoulder.
What are the symptoms?
Most common symptoms of a labral tear include a pain/ache that’s deep inside the shoulder joint, loss of velocity when throwing, and instability of the shoulder (feeling that the shoulder is going to ‘pop out’). Other symptoms include a popping or clicking sensation inside the shoulder, pain with overhead activity, pain in the front or back of the shoulder depending on where the potential tear is, and trouble sleeping at night.
How is a tear diagnosed?
The best way to diagnose a labral tear is seeking an evaluation from an Orthopedic Physician. The Orthopedic Physician will perform a clinical exam to evaluate for a tear. In order to do an evaluation, the Physician will perform several common orthopedic special tests that indicate a labral tear could be present. These common tests include Obrien’s test, Jerk test and Mayo test. Obrien’s test is performed in order to rule out a tear in the front part of the shoulder. Jerk test is performed to evaluate for instability in the back portion of the Labrum. The Mayo test is performed in order to evaluate for a Labral tear in the front of the shoulder as well.
If the physician suspects a labral tear, further imaging is needed to confirm the diagnosis. Further imaging in the form of an MR arthrogram is typically ordered. The MR arthrogram is a little different than a typical MRI because dye is injected into the affected joint. This dye adds to the imaging test because the fluid from the dye can sneak under the tear and make it easier to detect on the images. This is the best way to interpret a labral tear short of having surgery.
How is a labral tear treated?
Labral tears can be treated conservatively or surgically. Conservative treatment includes anti-inflammatory medication, physical therapy, steroid injections and rest. If conservative treatment doesn’t reduce the patient’s pain, surgical intervention may be necessary.
Surgical intervention means that an arthroscopic surgery will be performed to repair the labral tear. Anchors are used so that sutures can be passed through them in order to tie the torn Labrum back into the socket. The amount of sutures used depends on the size of the tear. If the tear is in the Bicep region, a procedure called an Open Subpectoral Bicep Tenodesis can be performed. This involves moving the Bicep Tendon to underneath a chest muscle so that the Bicep Tendon is no longer pulling on the front part of the Labrum.
Recovery from surgery:
Recovery from Labrum Repair surgery can take up to 6 months depending on the extent of the repair. Initially after surgery, the patient will be in a sling for 6 weeks. After that, the patient will have a lifting restriction of 5 pounds for the next 6 weeks and then a 10 pound lifting restriction for the 3 months following. At 6 months from surgery, the patient will most likely be cleared for all activity with the understanding that it may take up to a full year from surgery for the patient to feel fully recovered. Physical therapy is also required in order to regain the range of motion and strength that’s required for a full recovery.
When should you consider surgery?
A Labral Tear can only be “fixed” by having it arthroscopically repaired. The Labrum can also be a pain generator, therefore if Physical Therapy and Steroid injections can reduce the amount of pain, surgery may not be needed. If the pain is affecting activities of daily living and/or the shoulder joint is unstable, repairing the tear may be the best option. Talking with an Orthopedic Surgeon like Dr. Robert Rolf is the best way to determine the most beneficial treatment method.
Meniscus Tears in the Knee
March 17, 2017
What is a Meniscus Tear?
The meniscus is a cartilage cushion between the femur (thigh bone) and tibia (large lower leg bone). There are two menisci in each knee. The lateral (outside) meniscus is small c-shaped cushion, whereas the medial (inside) meniscus is a larger c-shaped cushion. Both menisci have poor blood supply and will not heal if they tear due to injury or degenerative causes. A meniscus tear typically occur when the foot is in contact with the ground and there is a twisting motion in the knee. Injury may also occur if the knee is forced to bend excessively (hyperflexion). The initial injury may or may not have associated pain; swelling typically does not occur until 48 hours after accident, and may not occur at all. Pain is generated after a tear when a piece of the meniscus folds on itself, causing catching, clicking, or popping in the knee joint. Most patients have difficulty going up and down stairs, and some may not be able to fully straighten or bend the knee.

www.tornmeniscusmd.com
How are Meniscus Tears Diagnosed?
Many meniscus tears can be diagnosed clinically based on history and physical exam. Special tests that are used for diagnosing meniscus injuries include McMurray Test, Bounce-Home Test, and Thessaly Test. A physician may order x-rays and/or MRI to help diagnose, or verify clinical suspicion of, a meniscus tear. X-rays may show decreased joint space between the femur and tibia. MRIs will show the location and type of meniscus tear and help the physician decide if the tear should be removed or repaired surgically. The MRI can also help with the decision to choose conservative treatment verses aggressive surgical intervention.
What is Conservative Treatment of Meniscus Tears?
Conservative treatment typically includes anti-inflammatory medication, physical therapy, and possibly a steroid injection in the knee joint (intra-articular corticosteroid injection). Conservative treatment will not repair a tear; this option manages symptoms.
What is Meniscus Surgery?
The majority of meniscus surgeries are menisectomies. A menisectomy is an arthroscopic procedure that allows the surgeon to identify the tear and trim the meniscus until it meets the tear, thus creating a new meniscus edge. Depending on the extent of tear and location of tear, the meniscus may also be repaired. This procedure can also be done arthroscopically, as the surgeon will use sutures to repair the tear. There is a risk that the meniscus may not heal due to limited blood supply.


www.drugs.com
Why Should I Consider Meniscus Surgery verses Conservative Treatment?
Meniscus tears will not heal on their own. Conservative treatment is beneficial to patients that do not have a decrease in motion in their knee. Anti-inflammatories can help control the pain that may be associated with the meniscus tear. Surgical treatment will remove or repair the tear.
What are my restrictions after a Meniscus Surgery?
Removal of the meniscus tear leads to limited healing time. Most people can be active in their normal routine within 6-8 weeks. Physical therapy will start almost immediately following surgery, and crutches can be used for up to a week. Repair of a meniscus tear has a longer return to activities of daily living. There is a risk of tearing the sutures used to repair the meniscus, therefore the patient is usually in a straight leg brace and non-weight bearing using crutches for at least 3 weeks. Hyperflexion or hyperextension (straight leg) can cause the sutures to catch on the femur and possibly ruin the repair. Recovery after a meniscus repair may take 3-6 months. Physical therapy for both surgical options involves strengthening of the quadriceps and hamstring muscles
What are the risks of Meniscus Surgery?
Complications are rare, but the potential does exist. Common complications may include: infection, decrease range of motion in the knee, rupture of repair, and swelling. Benefits of meniscus surgery commonly outweigh the risks.
Written By: Lisa Osterbrock, PA-C, ATC 9/18/14
Edited By: Robert Rolf, M.D.
What is a Biceps Tendon Rupture and How is it Fixed?
March 17, 2017
The biceps muscle group (biceps brachii) is made up of two heads, the long head and the short head. The muscles originate at the shoulder and insert on the radius (short bone in the forearm). The main function of the biceps brachii is to supinate the forearm (pretend like you are holding a cup of soup in the palm of your hand; this position is called “supination”). The second function of the biceps brachii is to flex (bend) the elbow. Rupture of the biceps tendon can occur proximally (at the shoulder) or distally (at the elbow). Ruptures commonly occur when there is an unexpected force applied to the bicep muscle such as attempting to catch something or someone when they fall. Most ruptures occur when the elbow is in a flexed position. Some people may feel or hear a “pop” when the tendon separates from the bone.


How is a Biceps Tendon Rupture diagnosed?
Ruptures of the biceps tendon can usually be diagnosed through history and physical exam. Observation of the injured extremity may reveal significant bruising and swelling, as well as physical deformity. The physical deformity associated with biceps ruptures is termed popeye deformity. The deformity is due to the tendon retracting toward the muscle belly causing a large bulge. X-rays may be ordered to rule out an associated avulsion fracture. An MRI may also be ordered to aid in visualizing the amount of damage sustained to the muscle, tendon, and bone.


Image courtesy of mdguidelines.com Image courtesy of eorthopod.com
What is Biceps Tendon Repair surgery?
Distal biceps tendon ruptures typically require surgical fixation to restore range of motion and strength to the elbow. This procedure is an open surgical procedure which can be performed on an outpatient basis. The goal is to reattach the tendon to the radius bone using either sutures or anchor with sutures.


Proximal biceps tendon ruptures can be treated conservatively with physical therapy and anti-inflammatories. Surgery is considered when a patient continues to have pain despite conservative measures. The biceps tendon is not reattached to its original origin; the biceps is attached to the humerus in a procedure called a “biceps tenodesis.”

Why should I consider Bicep Tendon Surgery?
Distal repair for a biceps tendon rupture should be considered in patients that injure the bicep in their dominant arm, or active individuals. The goal of surgery is to restore strength and endurance to the musculature as well as maintain range of motion in the elbow joint. Without surgery, there is a significant probability that function of the injured extremity will be limited. Proximal bicep tendon repair is considered when conservative measures fail or do not relieve pain.
What are my restrictions after a Bicep Tendon Surgery?
Total healing time for any injury or surgical repair is usually one year. Limitations vary based on distal or proximal repair. Both repairs for a biceps tendon rupture will require the use of a post-operative sling for up to 4 weeks. Physical therapy will begin range of motion and strengthening activities based on protocols established by Dr. Rolf, or your preferred surgeon.
What will be my recovery time?
Distal and proximal bicep tendon repairs are performed as an outpatient surgery. Formal physical therapy can begin within 2 days of surgery. Formal therapy can last 12-16 weeks with gradual progression to a home exercise program. Most patients are able to return to normal activity, without restriction, 14-20 weeks after surgery. The variable wide range of return to activity is based on a distal or proximal bicep repair.
What are the risks of surgery to repair a biceps tendon rupture?
Complications associated with bicep tendon repair are rare. Common risks associated with a distal repair include: decreased strength, decreased nerve sensation, and decrease range of motion at the elbow. Common risks associated with proximal repair include: decreased strength, decreased nerved sensation, and decreased range of motion at the shoulder. Both surgical techniques have associated risk of pain, infection, and slow wound healing.


Written By: Lisa Osterbrock, PA-C, ATC
Edited By: Robert Rolf, M.D.
Images courtesy of proactivept.com, eorthopod.com, and mdguidelines.com.
Shoulder Impingement
March 15, 2017
What is a Shoulder Impingement?
Shoulder impingement occurs when the tunnel between acromion process off of the shoulder blade and the humeral head is small or the structures that run through the tunnel are inflamed. The tunnel is known as the subacrimial space. The structures that become inflamed are the subacromial bursa, supraspinatus muscle, and/or biceps tendon (long head). The subacromial bursa is a fluid filled sac that prevents wear and tear of muscle tendons as they move around a bone. The supraspinatus muscle is the main rotator cuff muscle that originates on the top of the scapula (shoulder blade), runs under the clavicle (collar bone), and inserts on the humeral head. The biceps tendon can pinch between the clavicle and humeral head. Impingement injuries commonly occur in patients that participate in overhead activities (working on ceiling fixtures, throwing motions). Overuse leads to inflammation causing a pinching pain when the arm is lifted above the head or brought across the front of the body.

http://morphopedics.wikidot.com
How is Shoulder Impingement diagnosed?
Shoulder impingement is a clinical diagnosis based on history and physical exam. Special tests that are used for diagnosing shoulder impingement include Neer’s, Hawkins-Kennedy, and Speed’s tests. Diagnostic testing may include x-rays or MRI to help rule out involvement of surrounding structures or other injury.
How is Shoulder Impingement treated?
Conservative treatment typically includes anti-inflammatory medication, physical therapy, and possibly a steroid injection (intra-articular corticosteroid injection) in the subacromial joint space. Range of motion is limited so that movement of the shoulder is pain free. The patient may be limited, not permitting the patient to lift their arm above shoulder level. Lifting the arm above shoulder level pinches the anatomic structures leading to inflammation preventing resolution of impingement.

Is surgery required for Impingement?
Surgery is not required for impingement. However, if conservative treatment fails, and the patient is still having significant pain, elective surgery may be the next option. Surgical options include a distal clavicle resection, subacromial decompression, and/or bursectomy, all of which are arthroscopic procedures. Distal clavicle resection removes a piece of bone from the clavicle; this allows an increase in size of the space below the clavicle decreasing pressure on the underlying anatomy. Subacromial decompression removes the undersurface bone from the acromion, which may include bone spurs (increased calcium formation). This procedure opens the subacromial space allowing the biceps, supraspinatus, and bursea to move freely without friction, thus preventing inflammation. A bursectomy is the removal of a bursea sac; for impingement, the subacromial bursea is removed.

www.methodistorthpedics.com
What are my restrictions after Impingement Surgery?
Patients will be immobilized with the use of a post-operative sling immediately following surgery. The sling is provided to decrease stress on the shoulder while healing occurs, as well as aid in decreasing soreness. Physical therapy will start within the first week following surgery, beginning with simple range of motion exercises and basic strengthening techniques. A patient can expect to be removed from the sling within 4 weeks of surgery, and have normal range of motion within 3 months. Pain is the most limiting factor following surgery for impingement
What are the risks of Impingement Surgery?
All surgeries have associated risks. Luckily, impingement surgery has few complications and the benefits typically outweigh the risks. Common risks and complications include bleeding, infection, swelling in the elbow/wrist/hand, and numbness/tingling in the elbow/wrist/hand.
See if you’re dealing with shoulder impingement and what the next steps are, by scheduling an appointment with Dr. Robert Rolf.
Common Questions About MCL Knee Sprains
March 15, 2017
What is a MCL Sprain?

MCL stands for medial collateral ligament and is located on the inside of the knee. The MCL originates on the femur (thigh bone) and inserts on the tibia (large bone of the lower leg). The MCL splits slightly at the knee joint and some fibers also insert onto the medial meniscus (cushion inside the knee). Due to attachment of the MCL on the medial meniscus, MCL sprains may also have an associated medial meniscus tear. An MCL sprain occurs when there is a direct force applied to the outside of the knee, pushing the knee inward. MCL sprains may also occur when a person sustains an ACL (anterior cruciate ligament) tear. There are 3 grades of sprains. A grade one sprain involves stretching and minor tearing of the MCL fibers; a grade two sprain involves partial (50%) tearing; and, a grade three sprain is a complete tear or rupture of the MCL. After sustaining any type of MCL injury, there may be difficulty bending and straightening the knee.
How are MCL Sprains diagnosed?
MCL sprains can usually be diagnosed clinically via physical exam. The health care provider will perform a special test called a valgus stress test. This test may reveal pain and/or instability on the medial side of the knee. X-rays may be ordered which may reveal an avulsion fracture; this involves the MCL pulling a small chip of bone off of the femur. A MRI may be ordered to verify the extent of tearing that has a occurred to the MCL and will also diagnose any additional associated injuries.
How is an MCL Sprain treated?
Most MCL sprains will heal with conservative treatment. These sprains include grade one and grade two sprains. Conservative treatment involves non-weight bearing with the use of crutches until the patient is able to walk without a limp or pain, and physical therapy to strengthen the surrounding musculature (quadriceps, hamstrings, adductors (groin)). The patient may also be placed in a hinged knee brace to help protect the knee from side to side motions. A grade three sprain/tear may require surgical repair.
Why should I consider MCL Surgery?
If someone has a complete tear of the MCL conservative treatment may be an option. The leg would have to be placed in a knee immobilizer, typically locked in full extension, for several weeks to allow scar tissue to form and repair the MCL. After scar tissue has formed, the patient will need to attend physical therapy to strengthen the surrounding musculature. Surgical treatment involves repair of the MCL or reattachment of the ligament to the bone. Surgical repair is not done arthroscopically; it is an open procedure. Surgical repair is preferred for athletes that require excessive amounts of twisting and pivoting at the knee joint.
What are MCL surgery post-surgical restrictions and recovery?
Following MCL surgery, the patient will be placed in a knee immobilizer that is locked in slight flexion (bent knee). The brace can be unlocked at the discretion of the doctor and physical therapist. With the brace locked in flexion, the patient will be non-weight bearing with the use of crutches for 4-6 weeks. The brace can be slowly unlocked to increase range of motion at the knee at the doctor or therapist’s discretion. Once the patient is permitted to weight-bear, strengthening, range of motion, and balance, are key areas that are addressed in therapy. Aggressive therapy usually does not occur until 12 weeks after surgery. It is important to realize that it may take up to a year for a patient to have full recovery following surgical repair of the MCL.
What are the risks of MCL Surgery?
Complications or risks are associated with any surgery. Common risks include: infection, loss of range of motion, and instability. In most cases, the benefits of surgery out weigh the risks.
Written by: Lisa Osterbrock, PA-C, ATC 9/23/14
Edited by: Robert Rolf, M.D.
Shoulder Sling Education (Breg SlingShot™ 3)
May 6, 2016
The SlingShot™ 3 Brace is a shoulder sling manufactured by Breg.
The brace is specially designed to hold the arm in the correct position to ensure that it heals quickly and correctly. Patients usually wear the brace for 4-6 weeks following surgery, and longer in some cases. One of the primary reasons your doctor selected this case is comfort. If you are experiencing discomfort, please contact your physician, or Breg directly.
Typical shoulder braces have straps that run across the back of the neck, putting extra pressure and weight on the spine. The straps can cause rubbing, digging, and irritation on the neck. The unique design of the SlingShot™ 3 means greater comfort because it moves pressure away from the neck. The fabric is thin, about the thickness of a dime (2mm) to ensure it is lightweight and breathable. There is also mesh fabric to keep the patient’s arm cool and reduce perspiration. Typical slings have fabric at the elbow, which often irritates the ulnar nerve. With this sling, however, the elbow is left open, and the strap can be adjusted.
Shoulder Sling Application and Care
After shoulder surgery, the doctor will put the shoulder sling on a patient. To remove the brace, make sure your injured arm is supported. Then you’ll unbutton the quick release buttons and gently slide your arm out of the sling. Sliding your other arm out of the harness should be easy. Don’t unbuckle any straps, and if your doctor has placed pillows in the brace, please try not to move them.
To put the brace back on, support the injured arm. Slide your injured arm’s forearm into the sling, then slide your other arm through the harness and slide it up onto your shoulder (similar to putting on a backpack). Attaching the closure strap across the top of the sling should complete the process. If you experience any increased pain or swelling or any other negative reactions at any time, please contact your doctor right away.
While SlingShot™ 3 is an amazing shoulder sling, it cannot protect your arm from everything. Re-injury can happen, so please remember to reduce your activity level, according to your doctor’s recommendations. Exercise appropriate caution when removing and applying the brace.
Taking care of the brace is easy. Just clean it periodically or as needed, depending on how active your lifestyle is and much you perspire. Hand wash it in cold water using a mild detergent. We recommend air drying after rinsing.
If you need a reminder on how to remove or put on the brace, either refer to the pamphlet that came with the brace, visit the Breg website, or use the QR code on the brace’s tag.
Trouble Shooting Your Shoulder Sling
The SlingShot™ 3 shoulder sling is designed to be comfortable and easy to use. There are a few things that might you find the perfect fit. Patients with larger chests may want to opt for the sling closure extension. This is available simply by contacting Breg and requesting one.
Pre-Operative Packets
October 5, 2015
Pre-Operative Packets:
Below you will find a list of Pre-Operative Packets for some of the common procedures performed by Dr. Robert Rolf. He specializes in elbow, hand, wrist, shoulder, knee, total joint replacements, and sports medicine. The pre-operative packets detail what to expect during and after common surgeries, as well as what to do and what not to do beforehand.
Surgery On Knee – Minimally invasive knee procedures.
Surgery On Shoulder – Minimally invasive shoulder procedures.
Surgery On Fracture – Open repair with hardware.
Surgery On Carpal Tunnel Trigger Finger
Surgery Total Knee Replacement – Total joint replacement of the knee.
Surgery Total Shoulder Replacement – Total joint replacement of the shoulder.
If you have additional questions regarding preparation for an operation, please give us a call at (513) 354-3700.
Physical Therapy Protocols – Dr. Robert Rolf
October 5, 2015
Below you will find a list of physical therapy protocols that can be followed after having a procedure performed by Dr. Rolf. These are intended to provide guidelines of progression in recovery. They include weight bearing status, ranges of motion, use of a brace, exercises or stretches, and other information.
AC Reconstruction – Protocols for shoulder surgery
Achilles Repair – Protocols for ankle surgery
ACL Protocol – Protocols for knee surgery
Arthroscopic Shoulder Capsular Release – Protocols for shoulder surgery
Arthroscopic Labral Repair – Protocols for shoulder surgery
Arthroscopic Partial Medial or Lateral Meniscectomy – Protocols for knee surgery
Arthroscopic Rotator Cuff Repair – Protocols for shoulder surgery
Arthroscopic Subacromial Decompression – Protocols for shoulder surgery
Anterior Stabilization – Protocols for shoulder surgery
DENOVO – Protocols for knee surgery
Distal Biceps Repair – Protocols for elbow surgery
Hemiarthroplasty for Proximal Humerus Fractures – Protocols for shoulder surgery
Interval Throwing Program – Protocols for shoulder surgery
Latarjet – Protocols for shoulder surgery
Lateral Epicondylitis Release – Protocols for elbow surgery
LCL Reconstruction – Protocol for knee surgery
MCL Repair with MPFL Repair – Protocol for knee surgery
Medial Patellofemoral Ligament Repair – Protocol for knee surgery
Meniscal Repair – Protocol for knee surgery
Nonoperative Management of Proximal Humerus Fractures – Protocol for shoulder fracture
ORIF Proximal Humerus Fracture – Protocol for shoulder surgery
Proximal Hamstring Repair – Protocol for hip surgery
Quadricep Tendon Rupture – Protocol for knee surgery
Reverse Total Shoulder Arthroplasty – Protocol for shoulder surgery
Reverse Total Shoulder Arthroplasty with Latissimus Dorsi Transfer – Protocol for shoulder surgery
Superior/Anterior Labral “SLAP” Repair – Protocol for shoulder surgery
Subpectoral Biceps Tenodesis – Protocol for shoulder surgery
Total Knee Replacement – Protocols for knee surgery
Total Shoulder and Hemiarthroplasty – Protocols for shoulder surgery
Pectoralis Repair – Protocols for shoulder surgery
Pectoralis Transfer – Protocols for shoulder surgery
Patellar Fracture with ORIF – Protocols for knee surgery
Sports Injury Prevention
October 5, 2015
Sports Injury Prevention: Stop the Injuries
In the world of orthopaedics, few things are as important as sports injury prevention. From pro athletes to competitive high school students to weekend warriors, most of us aren’t doing enough to prevent common sports injuries.
Below is a list of common sports and activities. Each link discusses some simple sports injury prevention methods. These are also helpful tips for parents and coaches. The organization STOP the Injuries is trying to lower knee injuries, stress fractures, ankle sprains, concussions, and other sports injuries among youth athletes.
The most common, and easiest to avoid, cause of sports related injuries is simply overuse. This often impacts volleyball players, baseball athletes, swimmers, and other sports involving repetitive motions, or use of the same muscles. Recognizing fatigue can also play an important role in sports injury prevention. When athletes begin to wear out, their technique often gets sloppy. This, too, can lead to pain. Please click on a link for more information.

Ankle Sprains
October 5, 2015
Rolled, Twisted and Turned: How to Get Back on the Court After Ankle Sprains
Rolled, twisted, and turned: three words that no one wants to associate with their ankles. All are common descriptions of ankle sprains. Ankle injuries can result in fracture, tendon injury, or most commonly an ankle sprain. There are an estimated one to 10 million acute ankle injuries in the United States on a yearly basis with fractures accounting for only 15 percent. (Berkowitz & Fierstein, 2011).
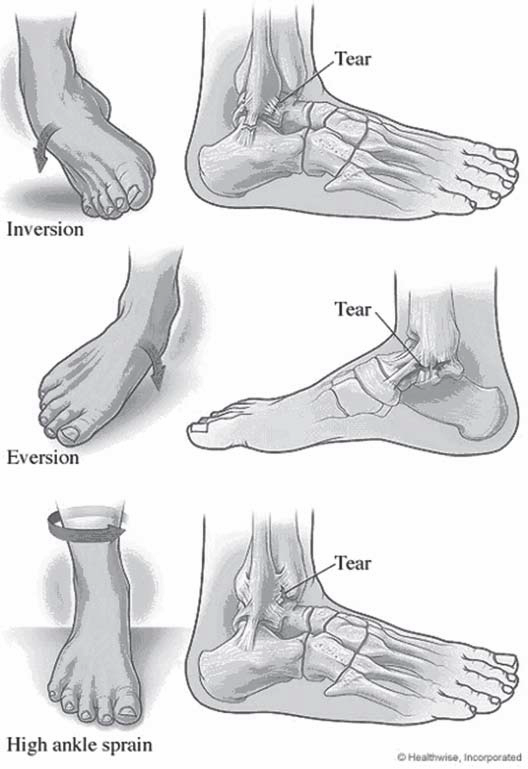 Ankle sprains are typically evidenced by pain and swelling in the ankle. A popping or snapping sensation may be felt and the person may have difficulty with bearing weight. Bruising is also common but may not be visible until hours or days after injury. The good news about ankle sprains is that most resolve with rest and support, however, what differentiates the ankle sprain that can be “walked off” almost immediately from the sprain which requires immobilization or surgical intervention? What type of support and treatment result in faster returns to activity or work?
Ankle sprains are typically evidenced by pain and swelling in the ankle. A popping or snapping sensation may be felt and the person may have difficulty with bearing weight. Bruising is also common but may not be visible until hours or days after injury. The good news about ankle sprains is that most resolve with rest and support, however, what differentiates the ankle sprain that can be “walked off” almost immediately from the sprain which requires immobilization or surgical intervention? What type of support and treatment result in faster returns to activity or work?
The ankle is a complex joint where the tibia (shin) and fibula (small bone of the outer leg) meet the talus (upper-most bone of the foot.) This joint is stabilized by three main ligament complexes. The most commonly injured are those of the outside or lateral ankle. These include the anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and posterior talofibular. These are typically injured when someone lands or rolls on the outside of their foot causing what is known as a forced inversion injury.
The inner ankle is stabilized by a number of ligaments known collectively as the deltoid ligaments. These are more commonly injured when a person rolls or land on the inner foot causing a forced eversion injury. This type of injury is also more likely to cause a fracture. The third set of ligaments is between the two bones of the lower leg and is known collectively as the syndesmosis. A high ankle sprain refers to injury to this syndesmosis.
Ankle sprains are typically diagnosed by a good history and physical examination. The physician will ask about the mechanism of injury and symptoms from the time of injury. They will examine the ankle to see where it is most tender and stress the ligaments to assess for any instability. They should also check the function of nerves and blood vessels that travel to the foot for any possible injury. X-rays may be necessary to rule out a fracture.
The Ottawa Foot and Ankle rules are a commonly used guideline for obtaining x-rays in acute injury. These guidelines state that x-rays should be obtained if the patient has tenderness over certain bone structures (medial malleolus, fifth metatarsal, or novicular), or if the patient is unable to bear weight immediately after injury or at time of examination. These are tailored to use in the emergency department and other guidelines may be used by an orthopedist or primary care provider. In those with persistent pain, an MRI to further evaluate the soft tissues may be needed.
Ankle sprains range in severity much like any other injury. Some are minor enough that even hours after injury the patient feels better. Others may last for weeks or require surgical intervention. The degree of pain and dysfunction is generally attributed to the amount of damage to the ligament or ligaments. Different grading systems can describe these in different manners.
No matter the severity of the sprain, the first measures of treatment are typically conservative. RICE (rest, ice, compression, and elevation), therapy can be helpful initially to help with pain relief and control of acute swelling. Anti-inflammatories such as ibuprophen or naproxen have also been traditionally used for pain and inflammation control. This has become more controversial in recent years as newer studies suggest that NSAID use may delay healing as inflammation is the body’s natural response to an injury in that it causes chemical signals in the body to recruit nutrients and growth factors to the site of injury. It is theorized that blocking this initial inflammation may lead to delayed healing.
Another traditional form of treatment for ankle sprains has been splinting or rigid bracing for immobilization. More recently there has been a rise in functional treatment for Grade I and Grade II sprains. Functional treatment typically consists of support with a lace-up or semi-rigid brace coupled with early physical therapy exercises to restore motion and strength. Ivins, et. al, showed people returning to sports 4.6 days sooner and work 7. 1 day sooner with functional treatment. Another study (Kerkhoff’s et. al, 2009), shows that more patients return to sport 4.88 days faster, and return to work 8.23 days faster. In general, they found that more people returned to sport in the long run.
Ankle therapy includes general range of motion as well as strengthening about the ankle. This is often combined with something referred to as proprioceptive training. Proprioception is the ability for a person to sense where they are in space. This is what allows us to catch objects in the air or step up and sown meeting the floor without falling. The nerve fibers that give us this sense are often impaired due to the ankle sprain often requiring retraining to prevent further injury from new falls or awkward positions.
Common ankle exercises for both treatment and prevention of an ankle sprain include range of motion exercises, which can simply be performed using a cloth or towel wrapped around the foot with the ends firmly in both hands. Gently pull the towel toward the face and hold for 15-30 seconds. This can be varied by also pulling with an inward roll of the ankle and outward roll of the ankle. These can be repeated 3-5 times. Also, you can perform a standing calf stretch by bending the knees while standing with their heels on the floor. Another creative way to work on ankle range of motion is to spell the alphabet with the great toe by moving the ankle through different planes.
Once you have full range of motion, strengthening exercises can be started to help prevent re-injury. Simple exercises can include pushing downward, upward, inward and outward on an immovable object holding each for 5 second for 10 sets. Then dynamic (moving), strengthening using the other foot, rubber tubing or weights can include the same motions, but instead of pushing and holding, this includes fully contracting the muscles over 1 second followed by taking 4 seconds to relax the ankle for three sets of 10 repetitions. Using the toes to pick up small objects and walking forward and backward on toes and heels are also common strengthening exercises.
Proprioceptive training is typically started when the patient can weight bear without much pain. This can be as simple as heel raises and toe raises or as involved as using a wobble board as well as walking on different surfaces (Berkowitz & Fierstein, 2011). Proprioception is also improved with single leg balance and using a jump rope. Formal physical therapy is often needed to initiate different exercises although most can be done at home. A good strengthening program helps facilitate your return to the court.
Achilles Injuries
October 5, 2015
Preventing Achilles Injuries: What can go wrong on the court?
Most people are familiar with the great story of Achilles who was dipped into the River Styx to become invincible. Unfortunately, Thetis held him at the ankle and so is born the “Achilles heel.” According to Homer’s Illiad, Achilles was slain when Paris shot an arrow into his heel. Fortunately, flying arrows are rare in today’s world, but that does not mean that you are immune to Achilles injuries on the court.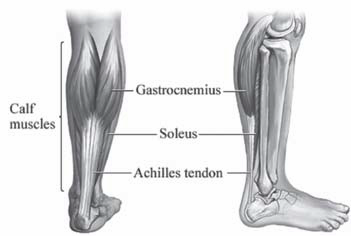
The Achilles tendon inserts on the back of the heel (or the calcaneus). It is comprised of two muscles (the gactrocnemeus and the soleus) which merge to become one tendon. It becomes round and then flattens about 4 cm. proximal to the heel. There are essentially four Achilles injuries that can arise with the tendon: Achilles tendinitis and tendinosis, paratenonitis, insertional tendinitis and Achilles ruptures.
Achilles Tendonitis
Achilles tendonitis is a condition when the Achilles is irritated and inflamed. There is a relatively avascular zone in the Achilles tendon that is roughly 2-6 cm. for the insertion of the Achilles into the heel. It is a common injury in recreational athletes and occurs when there is overuse of the tendon that causes inflammation leading to pain and swelling. When the condition is chronic, it leads to Achilles 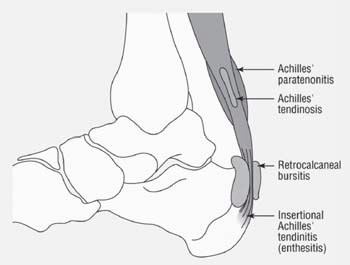 tendinosis. With tendinosis, there are microscopic tears within the tendon. The paratenon is a sheath that envelopes the tendon. It can become inflamed with repetitive strain or overuse. The tendon may also be thickened. The pain improves with rest and is aggravated with activity. It tends to be associated with overuse and is not a precursor to Achilles ruptures. Insertional tendinitis is characterized by inflammation and pain surrounding the point where the tendon inserts into the heel. This can lead to partial tearing or rupturing of the tendon. A person will complain of tenderness directly over the Achilles insertion into the heel and can make weightbearing difficult. The tendon can become hardened and thickened. Surgery may be necessary for those cases recalcitrant to nonoperative treatment such as rest, cross-training, anti-inflammatories, stretching, and physical therapy.
tendinosis. With tendinosis, there are microscopic tears within the tendon. The paratenon is a sheath that envelopes the tendon. It can become inflamed with repetitive strain or overuse. The tendon may also be thickened. The pain improves with rest and is aggravated with activity. It tends to be associated with overuse and is not a precursor to Achilles ruptures. Insertional tendinitis is characterized by inflammation and pain surrounding the point where the tendon inserts into the heel. This can lead to partial tearing or rupturing of the tendon. A person will complain of tenderness directly over the Achilles insertion into the heel and can make weightbearing difficult. The tendon can become hardened and thickened. Surgery may be necessary for those cases recalcitrant to nonoperative treatment such as rest, cross-training, anti-inflammatories, stretching, and physical therapy.
Achilles Tendon Ruptures
Achilles tendon ruptures can occur in the substance of the tendon (in the avascular zone) or they can occur where the tendon avulses off the calcaneus. They are up to 12 times more common in men than women and usually result from noncontact injuries where the load to the Achilles exceeds the strength of the tendon. This can result from mechanisms such as a forceful push-off of the foot with an extended knee (jumping or sprinting), sudden unexpected ankle dorsiflexion, or violent dorsiflexion of a plantar-flexed foot.
Many times, a person may feel like they got kicked in the back of the heel by someone. The immediate pain is shortlived, but people will notice the inability to push the heel off the ground when walking. There may be swelling and/or bruising. Sometimes, a person may notice a palpable defect in the tendon. It is usually difficult to walk. When a physician squeezes the calf in the normal ankle, the foot will dorsiflex or flex down toward the ground. When the same test is done in the injured leg, there is no movement at the ankle. This is called a positive Thompson test. Achilles ruptures are almost always diagnosed clinically, but when there is uncertainty, an MRI is an excellent test to evaluate the integrity of the Achilles tendon.
Despite recent attention to surgical treatment of Achilles ruptures, the decision to treat these injuries surgically versus nonoperatively remains controversial. Nonoperative management is historically associated with a high risk of Achilles rerupture, ranging from 13 to 30%, but without wound complications. Operative management of Achilles tendon ruptures results in a lower re-rupture rate (0 to 6%), earlier mobilization, and better return to sports, but with the risk of higher wound complications (up to 21%). Recent studies suggests an infection rate that is much lower.
The goal of surgical management is early mobilization to maximizes healing potential. This requires strong suture material and a sound technique. Two such techniques include the Krackow suture and the “Giftbox” technique. as described by
Labib, et al.
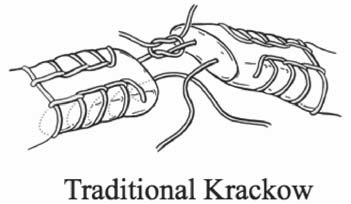
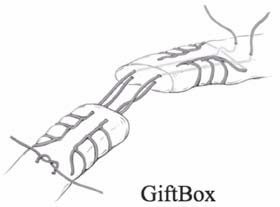
After surgery, the repair is splinted for up to two weeks with no weight bearing. Thereafter, the heel is placed in a boot with heel lifts that are removed over the next month. Weight bearing usually begins around two weeks, although this may vary depending on the surgeon.
Achilles injuries occur as a result of being in the right situation at the wrong time. That is, the force applied to the tendon is stronger than the tendon can withstand. Sometimes, that just cannot be prevented. Achilles tendon injuries such as tendinitis, insertional tendinitis, tendidnosis, and paratenonitis typically respond well to nonoperative management.
Prevention of Achilles Injuries:
As people age, calf and Achilles tightness is almost inevitable due to several reasons. First, as we become more sedentary, we have less daily stretch of the calf muscles and Achilles tendons. There is also age-related decrease in the elasticity of the Achilles tendon. Finally, higher-heeled shoes put the Achilles tendon in a shortened position. A good stretching and strengthening program is the best way to prevent Achilles injuries.
Achilles tendon stretching will result in satisfactory relief in better than 90% of the people suffering from Achilles pain. Some
people require as little as 3 weeks to see improvement while others may need upwards of 5-6 months to break through a long standing Achilles contracture. The heel stretching protocol is outlined below in detail. In the beginning, the amount you stretch will vary due to pain or soreness of the Achilles. Be sure to stretch both feet.
First of all, you will need a step to stand on with a wall for support. A routine step lift works extremely well. With your back against the wall and your knees straight, place the balls of your feet on the step and slowly relax your ankles, letting your heels go downward (see figure). You should not be gripping the step with your toes. If you are in the correct position, you should feel a pulling or tightness in your upper calf muscle, just below the knee. This should be tolerated until slight pain is felt.
For best results, do the stretch three times per day, gradually increasing the amount of time. You may need to stay at the same amount of hang time for a few days. Increase your time gradually, maxing out at three minutes. This is a gradual process and be patient. If you go right to three minutes, you may cause yourself more pain. Be Patient!
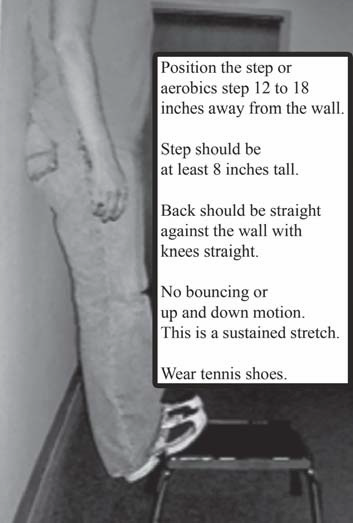 Week I – 15 seconds, 3 times/day
Week I – 15 seconds, 3 times/day
Week II – 30 seconds, 3 times/day
Week III – 1 minute, 3 times/day
Week IV – 1 1/2 minutes, 3 times/day
Week V – 2 minutes, 3 times/day
Week VI – 2 1/2 minutes, 3 times/day
Week VII – 3 minutes, 3 times/day
Hand Only CPR: A Better Way to Save Lives?
October 5, 2015
Hand Only CPR: A Better Way to Save Lives?
Out-of-hospital cardiac arrest affects more than 300,000 people annually in the United States. It is certainly something that could happen on the handball court. When this happens, the heart stops beating. A person usually collapses, stops breathing and is unresponsive. Since survival is so strongly dependent on immediate action by bystanders, what if we could increase survival odds through hand only CPR?
Although conventional CPR (chest compression and rescue breaths) can double the survival rates of victims having cardiac arrest, only one third of the victims have someone attempt CPR. The most common barrier to bystander action is the their concern for disease transmission as a result of mouth-to-mouth resuscitation. Another barrier is the fear of harming the victim from inadequate training. Much attention has been given to eliminating the barriers and getting more people to help begin resuscitation.
Hand only CPR (chest compressions only) has increased bystander involvement as well as survival rate. Several studies have shown that hand only CPR can be as effective as conventional CPR in the out-of-hospital setting. As a result, The American Heart Association released an advisory statement supporting hand only CPR in an attempt to increase bystander response to victims suffering from cardiac arrest. In fact, people were more likely to perform hand only CPR over conventional CPR regardless of their basic life support training. A study out of Arizona supports hand only CPR over conventional CPR. After looking at 4,415 adult cardiac arrests outside of hospitals from 2005 to 2009, researchers found that the rate of bystanders attempting CPR increased from 28% in 2005 to 40% in 2009. People were more likely to use hand only CPR.
In addition, victims were more likely to survive. Thirteen percent (113/849) of victims who received hand only CPR survived compared to eight percent (52/ 666) who received conventional CPR. In a recent study in The Lancet, three studies were combined and showed a survival rate of 14% for hands-only CPR versus 12% for conventional CPR. The authors recommended that rescuers should focus on hand only CPR with out of hospital cardiac arrest. So how do you do hand only CPR? First, if someone collapses, call 911 or have someone else call for you. Then get directly over the victim, lock your elbows and push hard in the center of the chest with both hands at a rate of approximately 100 times per minute. If you know standard CPR, then include rescue breaths. If an AED is available, switch it on and follow the instructions. Remember, any attempt at CPR is better than no attempt. According to the American Heart Association, hand-only CPR is recommended for use in adults who suddenly collapse. Conventional CPR is still recommended for “all infants and children, adults already found down or not breathing normally, and any victims of drowning or collapse due to breathing problems.”
Automatic Electronic Defibrillator (AED) Cardiac arrest usually results from an abnormal heart rate called ventricular fibrillation. It can happen to anyone at anytime. A automatic electronic defibrillator (AED), gives a victim an electronic shock that corrects the ventricular fibrillation by interrupting the irregular rhythm of the heart, reestablishing the normal electrical rhythm. An AED is a device that allows a person to monitor the heart rhythm of a victim and delivers a shock if necessary to re-establish the normal rhythm. Using AEDs with CPR quadruples the survival rate compared with using CPR alone. AEDs are easy to use. and all of them come with instructions that should be used. Place one pad on the upper right chest and one pad on the lower left side. If the electrodes are not attached properly, there is usually an error message. When the AED is attached properly, it will prompt you to analyze the rhythm. If the heart rhythm requires defibrillation, you will be prompted to do so. Be certain nobody is in contact with the victim while administering the shock. A simple way to make sure that every is safe is to say “I’m clear, you’re clear, everybody clear!” There are some special considerations with AEDs. If the victim is hypothermic, it may take longer to assess for a pulse (up to 45 seconds). If patients have pacemakers or implantable devices, do not place the AED pads over the device. Some patients use nitroglycerin patches and these should be removed prior to applying the AED pads.
Shoulder Treatment Education
October 5, 2015
Why an Article on Shoulder Treatment Education?
Proper shoulder treatment education is important when you or someone you love has a shoulder injury. The shoulder is a very delicate joint. Simple tasks like picking up pans, opening a window, moving a chair, or carrying a child can cause shoulder injuries. Activities like tennis, football, volleyball, and martial arts can cause further shoulder damage. Unfortunately, simply aging can cause tendon pain in the shoulder. Below are some of the common treatment options. Shoulder treatment education would not be complete without mentioning some of our non-surgical options, but we will get into those in a later post.
What is Shoulder Arthritis?
Arthritis is a common disease that affects the shoulder, causing joint pain, stiffness and swelling. When a person gets arthritis, they lose cartilage or the cushion in the joint. Cartilage allows the joint to glide easily during motion. When cartilage wears, there is bone on bone rubbing which can be painful. In addition, the joint becomes inflamed and there is usually a restriction of motion.
How is Shoulder Arthritis diagnosed?
Many patients will complain of a deep ache that can radiate to the lateral arm. The pain usually gets worse with movement or activity. With time, there may even be pain at rest and eventually, patients will awaken at night with shoulder pain. Patients will complain of grinding and difficulty with motion. In the office, a physician will diagnose arthritis through a thorough physical exam and taking the proper x-rays.
What is Shoulder Replacement Surgery?
In total shoulder replacement, the damaged surfaces of the humeral head and glenoid socket are resurfaced with metal and plastic implants. The humeral head is replaced with a metal component and the glenoid socket is replaced with a polyethylene component that is glued in with bone cement. When both sides of the shoulder are replaced, it is called a total shoulder replacement. When only the humeral head is replaced, it is called a shoulder hemiarthroplasty or a partial shoulder replacement.
Why should I consider Shoulder Replacement Surgery?
Shoulder replacement surgery should be performed to alleviate pain and improve function. It is an excellent option for patients that have failed other conservative measures such as physical therapy and antiinflammatory medication.
How long will my Shoulder Replacement last?
Anytime implants are used to replace your normal anatomy, it is expected that they will wear with time. The survivorship of a shoulder replacement is up to 93% at 10 years and 87% at 15 years. (Torcia et al.) At one year from the time of surgery, 98.5% patients are glad they had the procedure done. Ninety percent of patients feel that their new shoulder has attained the 80 percent of what they feel a “normal” shoulder would be and 37 percent of patients think that their new shoulder is normal. (Warner et al.)
What are my restrictions after a Total Shoulder Replacement?
Most activities can be resumed after a shoulder replacement. A person usually resumes activities such as swimming, golf and tennis by six months after surgery. Activities that involve major impact (such as contact sports or those where falls are frequent) or heavy loads (such as lifting heavy weights) should be avoided since these may increase the chance of rotator cuff tears, hardware loosening, increased wear and/or fracture.
What will be my recovery time?
Patients whom undergo total shoulder replacement usually stay in the hospital for 1-3 days after surgery. Physical therapists will begin moving the shoulder on the first postoperative day and patients will wear a sling for the first 4-6 weeks. At that time, patients can use their shoulder as tolerated with a weight restriction of 5 pounds. Most activities can resume in 4-6 months.
What are the risks of Shoulder Surgery?
Complications are rare, but they are also real and do happen. Some of the more common complications include infection, stiffness, instability, component failure, fractures around the prosthesis and failure to get complete pain relief. Fortunately, the benefits of shoulder replacement far outweigh the risks.
What is the difference between a chronic torn rotator cuff and acute tear?
Do both require surgery?
An acute rotator cuff tear is a tear that occurs after an injury. There is usually sudden pain in the shoulder accompanied by limited movement and weakness. A chronic tear is a tear that is greater than 6 to 12 weeks old. They usually involve the dominant arm and gradually worsen. People may develop weakness. There are many functioning patients with chronic tears. At sixty, fifty percent of asymptomatic patients would have a partial thickness rotator cuff tear if they had an MRI. At 80, fifty percent of patients would have a full thickness tear (all the way through). Chronic tears usually require surgery if the patient has persistent pain or weakness despite 6-12 weeks of physical therapy. Most acute rotator cuff tears or tears in young patients should be fixed surgically.
Why do physicians recommend a total shoulder replacement now?
Ten years ago, I never heard of a total shoulder. Shoulder arthritis is a common disease affecting thousands Americans annually. Many people with shoulder arthritis will have adequate pain control and function using anti-inflammatory medication and physical therapy. For patients that fail to improve with non-operative management, shoulder replacement is an excellent alternative. Up to 40,000 shoulder replacements are performed annually. At one year from surgery, 98.5% patients state that they are glad they had their shoulder replaced and would do it again. The successful results of shoulder replacement are similar to those for hip replacement surgery.
Do you have to repair a torn bicep even if it was injured five months ago?
The biceps is a muscle on the front of the shoulder that allows a person to flex and supinate the elbow. It has two muscle bellies, the long head of the biceps that inserts on the labrum at the top of the shoulder socket and the short head of the biceps that inserts on the front of the scapula at its coracoid. At the elbow, the bicep muscle bellies merge into one tendon that inserts into the radius. When a patient ruptures the distal part of the biceps, they may lose up to 40% of their strength with flexion and supination. Surgery is typically recommended when it is the dominant arm and the patient’s job requires significant use of the arm. Surgery is not always recommended for ruptures that occur near the shoulder at the long head of the biceps. Most people respond well to physical therapy.
I am a senior and I don’t want surgery but I can’t lift my arm, would therapy help relieve the pain?
There are many reasons a person may have pain in the shoulder and not all of them need to be treated surgically. Most shoulder ailments improve with physical therapy. It is helpful to have a thorough physical exam so that physical therapy can be guided appropriately. Sometimes, a platelet injections (platelet injections) or steroid injection can be helpful.
We hope this shoulder treatment education article has been helpful! For any additional questions or treatment options, give us a call at (513) 354-3700 or schedule an appointment with Dr. Robert Rolf!