What is Turf Toe
September 14, 2025
Several things can cause great toe pain: arthritis, injury to the bone, and soft tissue. A turf toe injury is when the bottom of the great toe is injured, and the soft tissue has damage to it. This is accompanied by pain, and it usually is onset by a hyper extension injury where the toe has forcibly moved upwards. Commonly, football is an injury historically with the type of turf it is played on, but this has become less common. Now, this injury is seen in baseball players running around the bases, some soccer injuries, and trauma in general.

Watch as Dr. Miller breaks down Turf Toe injuries on the Bengals Beat podcast
The hallmark of a turf toe injury is pain on the bottom of the great toe and is caused by an acute injury. It is associated with swelling and there is sometimes bruising into this area and a general reluctance by the patient wanting to walk on it. This can often lead to a feeling as if you’re walking on the outside of the foot. When you can’t walk on your foot, generally an evaluation should be had, and Dr. Miller can see you and provide a good evaluation. When being seen for a turf toe injury, we will examine the foot in general to make sure there is nothing else going on. But the focus and concerns will be surrounding the bottom of the great toe. This is where the soft tissue could be injured or the sesamoid bones, which are accessory bones that work in conjunction with the soft tissue to provide stability and function to the toe. Think of this as the kneecap to your knee. The kneecap functions as a fulcrum to make the knee move better. It is attached to muscles and tendons which allow the knee to move which is similar to the toe with the accessory bones called sesamoids on the bottom of the toe. When this complex is injured, you have difficulty with pain and push off. People will also have instability where the big toe itself moves abnormally. This creates pain, but the increase in motion is not physiologically motion. This abnormal motion over time causes pain and results in wear and tear in the joint.

In most cases these injuries can be treated non surgically. They often take extensive protection and time. Some patients will start out in a boot and if the toe is stable overall where the soft tissue is injured partially or just a sprain of the tissue, this can be successful and appropriate shoe-ware and protection is provided. Often after the boot the patient will be transferred to an extension or carbon fiber plate insert for continued protection in a normal shoe as the patient starts to get back to normal activities. In mild cases, a couple weeks of protection may get the person back to playing sports. In more significant cases, several weeks can be the appropriate recovery period.

Surgical intervention is usually left for the complete tear or instability of the soft tissue where the turf toe is associated with a complete tear which is called a plantar plate. This is where the sesamoid is completely detached from the soft tissue that attaches to the bone of the great toe. Surgery involved repairing the soft tissue or even reconstructing it with the associated tissues around the toe.
Post operatively the patient is often non weight baring, initially walking on the heel after 2-3 weeks of protection. This is followed by walking in a boot and physical therapy to begin mobilizing the lower extremity. Usually, full impact is not recommended for 2-3 months following the injury.

If you believe you may be experiencing a turf toe injury or know someone he may, Dr. Miller is Beacon Orthopedics’ foot and ankle specialist and is available at several locations around the Cincinnati area. Contact us today for more information! Click here to learn more and schedule an appointment with Dr. Miller for foot and ankle injuries.
Beacon Earns National Recognition as a Stryker Center of Ankle Excellence
July 11, 2025
 Beacon Orthopaedics & Sports Medicine is proud to announce its designation as a Stryker Center of Ankle Excellence—a prestigious honor awarded to just 13 orthopaedic practices across the United States.
Beacon Orthopaedics & Sports Medicine is proud to announce its designation as a Stryker Center of Ankle Excellence—a prestigious honor awarded to just 13 orthopaedic practices across the United States.
What does this mean for our patients? It means that Beacon is now officially recognized as one of the top destinations in the country for total ankle replacement surgery—and the only Stryker Center of Ankle Excellence in Southwest Ohio, Indiana, and Kentucky.
This distinction reflects the exceptional experience and dedication of our foot and ankle team, which includes Dr. Adam Miller, Dr. Robert Raines, and Dr. V. James Sammarco. Together, they bring more than 70 years of combined clinical experience and have performed hundreds of total ankle replacements—helping patients get back to the activities they love with less pain and better mobility.

To earn this recognition, Beacon had to meet rigorous criteria, including:
- Employing at least three fellowship-trained foot and ankle surgeons
- Performing 60+ total ankle replacements per year
- Offering both primary and revision ankle replacements
“We are proud and honored to be recognized by Stryker Corporation as one of only 13 centers of excellence nationwide for total ankle replacement,” says Dr. Raines. “This designation reflects our long-standing commitment to clinical excellence and innovation in ankle care.”
Each of our physicians sees patients at multiple Beacon locations:
- Dr. Adam Miller: Erlanger, Hyde Park (Cincinnati Sports Club), Summit Woods (Sharonville), and Western Hills (Beacon West)
- Dr. Robert Raines: Anderson – Beechmont (Beacon East), Fort Thomas, and Western Hills (Beacon West)
- Dr. V. James Sammarco: Erlanger, Fairfield, and Montgomery

The only other designated Stryker Center of Ankle Excellence in Ohio is located in Columbus—also part of the OrthoAlliance network—further highlighting our role as a regional leader in advanced ankle care.
Whether you’re managing chronic ankle pain or exploring surgical options, you don’t have to travel far for world-class expertise. Beacon’s foot and ankle experts are here to help you get back on your feet—literally.
Is it a Broken Ankle or a Sprain?
December 8, 2024
You fall and injure your ankle. Next you gauge your pain and ask: “Is it a broken ankle or a sprain?” This scenario accounts for one of the most common complaints; yet a simple twist and fall could become a complex injury involving bone, cartilage, ligaments and tendons. In this blog I will discuss ankle fractures and what the next steps are on the road to recovery.
Key Takeaways
- Ankle injuries can range from sprains to fractures.
- A proper diagnosis is crucial for effective treatment.
- Treatment options include non-surgical methods like immobilization or surgical intervention.
- Recovery time varies depending on the severity of the injury and the chosen treatment.
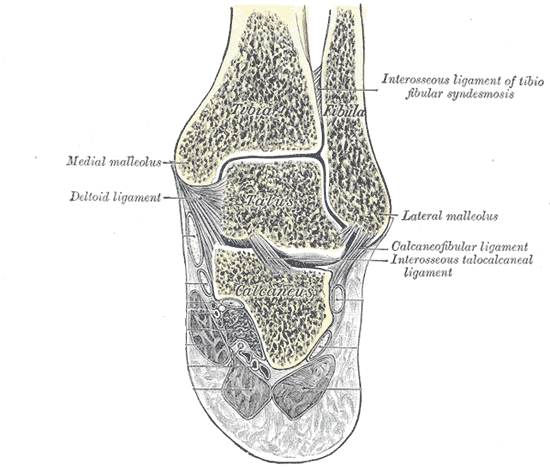
Ankle Anatomy and Injury
The ankle joint, composed of the tibia, fibula, and talus, is a complex structure. Ligaments, including the deltoid, lateral ligament complex, and syndesmosis, stabilize the joint. Injuries to these structures can result in pain, swelling, and limited mobility.
Diagnosing an Ankle Injury
A healthcare professional will assess the severity of the injury by considering factors like pain, swelling, and the ability to bear weight. Imaging tests, such as X-rays, may be necessary to confirm a fracture.
Pain free motion of the ankle relies heavily on this complex congruent relationship between the talus and the tibia and fibula. If the ankle joint is even displaced 1mm, a 42% increase in pressure to ankle may occur1. A change in the bony anatomy of the ankle involved with an ankle fracture may introduce enough change in alignment that the ankle is now at risk for future arthritis.
Is the Ankle Sprained or Broken?
 A thorough evaluation by an Orthopedic Specialist in Foot and Ankle such as Dr. Miller will identify the nature of the injury. Immediately following the injury, factors like pain, swelling, and the ability to bear weight will allow us to assess the severity of the injury. Imaging tests, such as X-rays, may be necessary to confirm a fracture.
A thorough evaluation by an Orthopedic Specialist in Foot and Ankle such as Dr. Miller will identify the nature of the injury. Immediately following the injury, factors like pain, swelling, and the ability to bear weight will allow us to assess the severity of the injury. Imaging tests, such as X-rays, may be necessary to confirm a fracture.
Swelling is another sign of injury. If the swelling comes on gradually and is mild, the injury is likely a sprain or less severe. More immediate and significant swelling indicates a bony injury and possible fracture. When severe fractures occur, blistering of the skin is not uncommon. The blisters emanate from excessive swelling in the soft tissues following a severe fracture. Sometimes the ankle is dislocated with this amount of swelling. Immediate medical attention is required in these circumstances to reduce the ankle. Once severe swelling or blistering sets in, this can take weeks until the initial swelling resolves. In many cases these changes can delay surgery on the ankle.
As time passes ecchymosis (bruising) may occur. This can be extensive; however, this does not necessarily mean the ankle is broken. More severe ankle sprains present with significant ecchymosis over the region of injury. Besides not being able to put pressure down on the ankle or a deformity in the ankle after injury, a good reason to be evaluated for a broken ankle/ankle fracture is continued symptoms that worsen or stay the same. Some ankle fractures are stable enough that you may still be able to walk. Some people have a high pain tolerance that allows them to cope with the injury. These scenarios are best evaluated by an orthopedic surgeon when not improving.
Orthopedic Evaluation
 Once you have made the decision to be evaluated for ankle pain, Dr. Miller will assess you and your injury as a whole. This includes a detailed history and physical examination with special focus on the ankle. Your age, mobility level and medical history are important, particularly as it relates to the ability heal an injury or recover from a potential surgery. Preexisting medical conditions such as diabetes, vascular problems, and inflammatory disease (e.g. rheumatoid) must be accounted for during the planning of treatment. Any remote history related to the ankle or previous injury should be known.
Once you have made the decision to be evaluated for ankle pain, Dr. Miller will assess you and your injury as a whole. This includes a detailed history and physical examination with special focus on the ankle. Your age, mobility level and medical history are important, particularly as it relates to the ability heal an injury or recover from a potential surgery. Preexisting medical conditions such as diabetes, vascular problems, and inflammatory disease (e.g. rheumatoid) must be accounted for during the planning of treatment. Any remote history related to the ankle or previous injury should be known.
Physical examination will be performed during your visit. It is important to assess the ankle based on its appearance including deformity, any open wounds around the ankle, the amount of swelling present, and any preexisting rashes or skin issues. Vascular exam is used to determine the appropriate blood flow to the lower extremity, and this is performed by checking the dorsalis pedis and posterior tibialis pulses surrounding the foot and ankle. A neurological exam of the lower extremity will be used to assess any nerve injuries and the ability to move the foot. The extremity will then be evaluated for areas of tenderness and pain. This will help to locate the injury in a broken ankle more specifically and rule out other concurrent pathology.
Findings from the physical exam will then be used to evaluate radiographs of the affected ankle and surrounding areas. X-rays consist of three views of the ankle and any other areas of concern. While minimizing radiation is a good general rule, lower extremity x-rays use very low levels of radiation and in comparison account for a small fraction of the radiation you naturally receive yearly by living on Earth2. Based on these images, Dr. Miller can evaluate for the presence of a fracture and the severity of the fracture.
Treatment
Once you have been identified to have a broken ankle/ankle fracture, how will the ankle be treated? Assuming you have an ankle fracture, the most important decision is whether the fracture can be treated non-surgically or the broken ankle requires surgical intervention. This decision would be made by Dr. Miller taking into account all variables described above.
In many cases the decision to perform surgery depends on the stability of the ankle. If 2 or more different fractures are identified in the ankle, surgery is commonly warranted due to the concern for instability and movement of the pieces. If the pieces heal non-anatomically, the ankle may be predisposed to accelerated wear and arthritis. If only one fracture is identified, the decision to perform surgery relies on the location and character of the fracture. Further radiographs that stress the ankle may be warranted to make this determination.
If the broken ankle has been considered stable enough to not require surgery, early weight bearing in a protective boot may be an option. This type of protection can be required for 6 weeks. You would wear the boot during all weight bearing activities. Usually at 6 weeks there is adequate healing to start weaning out of the boot.
If the broken ankle/ankle fracture is severe or unstable, surgical intervention utilizing metal implants is likely required. The day of surgery a patient typically will receive a nerve block prior to surgery that helps with anesthesia and pain control after the procedure. This process anesthetizes the leg to achieve temporary numbness. Once this is complete the actual surgery usually lasts between 1 and 2 hours. The surgery consists of reducing the broken pieces of the ankle to where they were prior to the injury and maintaining that reduction with metal hardware. Generally one or two incisions are used. A soft cast or splint would be applied for temporary protection until you return the office. After surgery it is imperative to elevate your leg to your heart level consistently until seen in the office. This improves pain relief and wound healing.

When you return to the office, the ankle is usually ready to be placed in a boot for protection. For the next 5-6 weeks no weight is to be put on the leg in most cases. One can start showering 2 weeks after the surgery on average. Around 6 weeks after the surgery, you can progressively apply weight to the leg while in the boot until you are completely weight bearing in the boot without an assist device. Range of motion and therapy begins 4-6 weeks after surgery. You can drive 9 weeks after surgery if your right leg was injured. Eleven to 12 weeks after surgery the boot is replaced with a shoe and possibly an ankle brace. Return to full impact and running would be achieved in the following months.
Appointments can be made with Dr. Adam G. Miller by calling (513)-354-3700 or booking online here.
1 Ramsey PL, Hamilton W. Changes in tibiotalar area of contact caused by lateral talar shift. J Bone Joint Surg Am. 1976 Apr;58(3):356-7. Epub 1976/04/01.
2 Coughlin MJ, Saltzman CL, Mann RA. Mann’s Surgery of the Foot and Ankle: Expert Consult-Online and Print: Elsevier Health Sciences; 2014.
Does Your Foot Hurt Here?: The Outside of the Foot
October 15, 2024
Ever felt a mysterious ache on the outside of your foot and wondered, “Why on earth does it hurt right there?” You’re not alone! Whether you’ve recently taken a tumble or the pain has snuck up on you, that outer edge of your foot can be a real troublemaker.

Picture your foot as a busy neighborhood, and that outer strip? It’s like Main Street, where all the action happens. From bones playing jump rope (hello, stress fractures!) to tendons throwing tantrums (we’re looking at you, peroneal tendonitis), there’s a lot going on in this tiny territory.
Today, we’re putting on our detective hats and diving into the most common culprits behind your outer foot woes. We’ll unravel the mysteries of Jones
fractures, decode the drama of tendonitis, and bust the myths around bursitis. So, grab a comfy seat, put that achy foot up, and let’s embark on a journey to the wild side (quite literally) of foot pain!
Jones Fractures
Jones fractures are a common fracture often brought on by injury and falling on the outside of the foot. This was named after the physician Dr. Robert Jones who described the injury in the 1900’s after sustaining one himself. The fracture occurs at the base of the fifth  metatarsal or the outside of the smallest toe. Sometimes these problems begin with a mild soreness before more significant pain develops. This is because they can be associated with stress to the foot. This area tends to lack blood causing these injuries to not heal very readily and sometimes not heal at all. These fractures will usually present with pain that comes on with walking traditionally, increased activity, or there truly is a twist of the foot and ankle onto the outside of the foot. Commonly, people will have pain and swelling, but in some cases, its pain and no swelling. Experiencing any ongoing pain in this area is worth an evaluation given the problems with healing.
metatarsal or the outside of the smallest toe. Sometimes these problems begin with a mild soreness before more significant pain develops. This is because they can be associated with stress to the foot. This area tends to lack blood causing these injuries to not heal very readily and sometimes not heal at all. These fractures will usually present with pain that comes on with walking traditionally, increased activity, or there truly is a twist of the foot and ankle onto the outside of the foot. Commonly, people will have pain and swelling, but in some cases, its pain and no swelling. Experiencing any ongoing pain in this area is worth an evaluation given the problems with healing.
These fifth metatarsal fractures, known as Jones Fractures, often need close attention and a follow up with an x-ray. Surgical intervention may be needed if it

is predicted that it won’t heal or will heal very slowly. Whether it be a person trying to get back to work or an athlete back to the field, intervening in this type of fracture may be crucial to a speedy recovery. Other recovery methods, depending on the results of the x-ray, might include wearing a boot for immobilization and instruction to be non-weightbearing. Surgery often involves either a screw or even a plate and screws depending on the severity of the injury.
Tendonitis
At the same exact location as a Jones Fracture, there is a tendon on the fifth metatarsal that moves the foot outwards. Tendons are similar to ropes. They connect muscle to bone and allow the foot and leg to move in certain directions. This tendon moves the foot from side to side and is called the peroneal brevis tendon. Because there could be injury to the tendon but not the
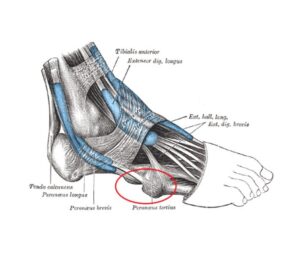
bone, there can still be pain but a completely normal X-ray. Often these problems will occur with no injury and come on over time with increased activity. Patients tend to feel pain and swelling on the outside of the foot. This pain may travel along the course of the tendon: the outside of the foot towards the heel.
People with a high arch are more prone to tendonitis because they put more of their body weight on the outside of their foot. This predisposes the tendon to having to work harder, therefore potentially having inflammation or even maybe a tear. To figure out what issue is going on with a perfectly clean x-ray, patients are given a trial of immobilization with a brace or a boot. Depending on the case, patients can also get imaging and MRI to delineate if it is a fracture or a tendon tear. If a boot or brace doesn’t help in the recovery process, physical therapy and/or anti-inflammatories can sometimes be used to alleviate pain and recover. In some cases, recalcitrant pain associated with the peroneal brevis tendon can signal a tear. This may require surgery for the pain to improve.
Bursitis
Sometimes patients will come in with generalized pain in the same area as tendonitis and Jones fracture due to overload on the side of their foot. This can be focal on the base of the fifth metatarsal, similar to a Jones fracture. However, it can also be more diffuse along the outside border of the foot. This pain is called bursitis because there is inflammation in the local tissue. Often over activity or constant pressure on the outside of the foot over time may cause this issue. Again the shape of the foot is a high arch in most patients. These patients put more pressure on the outside of the foot. These is often swelling or even callus formation on the bottom of the foot along the outside border. Usually pain is more along the bottom of the foot that the top.
on the outside of the foot over time may cause this issue. Again the shape of the foot is a high arch in most patients. These patients put more pressure on the outside of the foot. These is often swelling or even callus formation on the bottom of the foot along the outside border. Usually pain is more along the bottom of the foot that the top.
With these types of patients, there is an attempt to rebalance their foot. A properly fitted insert for a shoe may successfully offload the outside of the foot thereby reducing pressure and pain from the bursitis. Stretching of the ankle and calf is crucial to reduce undo pressure along the bottom of the foot. Anti-inflammatories are helpful when able to be taken safely. If pain continues, then it is important to follow up for a formal evaluation with imaging to make sure you obtain proper treatment.
We Are Here to Help
Do you have high arched feet? Are you experiencing any of these pains on the outside of your foot? Don’t wait, get an evaluation today! Dr. Miller is available here in Cincinnati’s own Beacon Orthopaedics. Contact us today for more information and schedule an appointment with Dr. Miller for foot and ankle injuries.
What to do about a bunion
April 1, 2022
Do I Have A Bunion?
People commonly notice a prominence with their big toe on the inside of their foot. In many cases this constitutes a bunion (hallux valgus). This can be unsightly and bother the patient. But it also can cause significant pain. Most commonly it causes pain while the patient wears shoes. Some shoes may be worse than others; however, tighter shoes may be more problematic. Historically, orthopedic foot and ankle specialists have often blamed the shoes for causing a bunion. There is some scant evidence for this, but in general we blame genetics for half of bunion formation. Environmental factors as the patient ages make up the rest that we don’t quite understand. In most cases, if your bunion is painful enough that it bothers you, then it is worth having Dr. Miller evaluate the pain and understand your options. 
Orthopaedic Evaluation Of My Bunion:
When a patient comes to the office complaining of bunion pain, the first thing Dr. Miller will do is have the patient stand and examine them. In most cases there is a deformity with potentially some redness from rubbing on the inside of the big toe. This is also met with the big toe sometimes impinging or resting onto the second toe. In more severe cases, the other toes can suffer a deformity over time as well. Additionally, we want to evaluate for any arthritis in the big toe which is where x-rays come in. We check the big toe for arthritis, deformity, and we identify and measure the severity of the bunion. This will help us determine if surgery is necessary and how to fix and correct the pain and deformity.
Types of treatment:
- Non-surgical: Initially, we always try non-surgical treatment and often the patient comes in having already tried what we recommend. Shoe changes and modifications to allow accommodation to the deformity is initially the first option. Sometimes taking the existing shoes and stretching them out or accommodating to the deformity with an insert is helpful. Sometimes it can be as simple as a pad in mild cases. There are several options for shoe protection, and it is something Dr. Miller as your orthopedic surgeon can go over. Sometimes an anti-inflammatory is effective and rarely injections are helpful because these are often temporary measures.

- Surgical: If non-surgical treatment has failed, then you and Dr. Miller may decide that surgery is the best option. This would be decided after discussion with Dr. Miller going over the risks and benefits of the procedure and any medical associated risk involved. Bunion surgery is an outpatient surgery and can be performed successfully in less than an hour and you’ll go home the same day. There are several different ways to correct a bunion. Dr. Miller will go over these options with the patient in detail to ensure they know what to expect. Based upon the examination and the imaging, the patient’s surgery is tailored to the foot and the deformity it presents. As the understanding of this deformity and technology has advanced, most patients can undergo bunion surgery now through a minimally invasive approach. Our patients have experienced early wound healing, early weight bearing, improved range of motion, and decreased post-operative pain when having the bunion corrected with a minimally invasive approach. Most patients can begin walking 2-3 weeks after surgery.



Post-Surgical Care:
After surgery the patient is asked to protect the foot with the dressings placed on the foot, elevate the lower extremity, and modify their activity. They are then seen back in the office within 1-2 weeks where dressings are changed, and further instructions are provided. Is it time to get your bunion evaluated? Contact Dr. Miller for honest expert opinion and advice. If someone you know is needing foot and ankle care, Dr. Miller specializes in foot and ankle orthopaedics and is available at several locations around the Cincinnati area. Contact us today for more information! Click here to learn more and schedule an appointment with Dr. Miller for your foot and ankle issue.
Winter Sports Blog
December 28, 2021
As colder weather approaches, we start to transition into the Winter months which brings in our winter athletes! This time of year, is very busy in the orthopaedic office where Dr. Miller sees many of his athletes participating in various sports including: hockey, basketball, wrestling, and gymnastics. Here we talk about many of the common injuries these athletes may endure during their Winter sports season.
Ankle Sprains:
Rotational injuries to the ankle or what we call an inversion injury, where the heel moves inside the leg, are the most common in Orthopaedics. Rotational injuries are most susceptible to athletes landing awkwardly and jumping in sports such as basketball and gymnastics. Also commonly seen in wrestling due to the number of awkward positions and manipulations of the extremities by the opponent. This injury is the third most common in wrestling following behind knee and shoulder injuries.
High ankle sprains:
In Ice hockey, due to the ankle being in a hard skate, the ankle is not able to roll (or invert) as much. We see rotational injuries where both the skate and the foot rotate externally, leaving the leg behind resulting in a high ankle sprain. A high ankle sprain is the injury to the ligament that goes up the leg connecting the big bone the tibia and the small bone the fibula. High ankle sprains can occur in any type of athletic activity but are seen most often in ice hockey. If seen in basketball, we recommend wearing high tops to increase the susceptibility to rolling the ankle.

Symptoms and treatment:
If an athlete believes to have rotated their ankle, lookout for signs such as swelling. If the swelling is coming on gradually and mild, the injury is likely an ankle sprain. With a more severe ankle sprain you may see significant bruising over the region of the injury. If the level of pain is severe, the athlete may get an evaluation with Dr. Miller to perform x-rays and determine the best healing process. To learn more about an ankle sprain refer to a past blog “Is it a Broken Ankle or a Sprain?”
Over-use:
An over-use injury is seen most in gymnastics with younger females who may not be fully skeletally mature or haven’t completely aged. Generally, females stop growing around 14 years old and males around 16 years old. Many teens will get pain along the growth plate in the calcaneus (heel) and it often comes on with impact, over-use, and repetitive activities. This may lead to growth pain/injuries known as Severs disease. The athlete may feel pain in the back of the heel, but after several hours of resting it begins to feel better. This is a repetitive injury as the athlete remains active. The only cure to this is aging however, along the way we recommend a lot of flexibility in the calf. This allows the Achilles tendon to pull less on the growth plate. Another option is offering a silicon cushion, heel cup as an additional protective layer. One recommended proactive measure would be giving the athlete an anti-inflammatory such as Motrin before their game or meet.

Sometimes pain does not go away with overuse and repetitive activities result in stress fractures. This type of pain may take weeks to improve with the right amount of protection. Appropriate immobilization includes boot therapy or brace.
Sesamoid injury:
Another repetitive injury is sesamoid pain which is common in wrestling and gymnastics with the athlete being barefoot. This causes lots of focused pressure on the ball of the foot under the big toe. This affects two little bones that are underneath the big toe, causing lots of swelling and pain in the area. To accommodate the injury, we try and offload this in a shoe. Also encouraging calf stretching to gain mobility while going up and not so much when the athlete lands and is coming down. More severe pain is amenable to temporary boot.

Accessory navicular bones
Has your athlete noticed a bump on the side of their foot getting irritated? Very common in ice hockey due to hockey skates being so unforgiving, the bump or accessory bone on the inside of the foot may be experiencing lots of pain due to exhaustion. Pain along the inside of the foot is often an issue with overuse in ice hockey due to the skate. Usually this can be accommodated by a custom skate fit if the athlete is consistently playing. If pain does not resolve, removal may be necessary for pain relief.

Trauma to the foot:
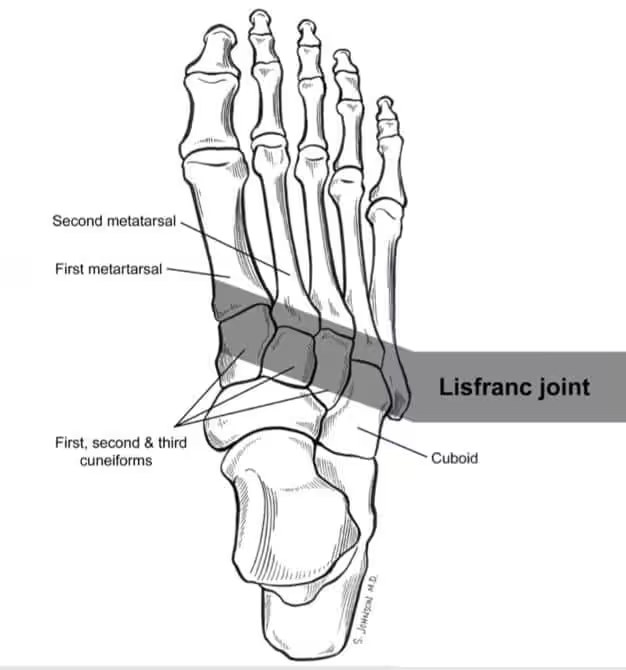
One very common injury Dr Miller sees is a Lisfranc injury. This is caused by an awkward landing when coming down, disrupting the axile impact. When athletes land, many times seen in basketball and most commonly gymnastics due to lack of shoe protection, the awkward landing causes the middle of the foot to twist inadvertently, potentially tearing the ligaments in your foot.

Symptoms:
What to look out for in potential injury is swelling, pain along the top of the foot, bruising seen on the bottom of the foot, and difficulty walking. A Lisfranc injury can be mild or more severe. Sometimes we refer to them as a mid-foot sprain and we declare as being stable which would require a boot therapy for treatment and improvement. Some we consider unstable after evaluation would need surgery. It is important to get a Lisfranc Injury looked at to prevent future collapse and arthritis. Tough to know without an evaluation! To learn more about a Lisfranc injury check out the Fall Sports Injuries blog. 
If you’re an athlete seeking for care do not wait, we are here to help! Dr. Miller is Beacon Orthopedics foot and ankle specialist and is available at several locations around the Cincinnati area. Contact us today for more information! Click here to learn more and schedule an appointment with Dr. Miller for your foot and ankle injuries.
Imaging in Orthopedics: What’s the right image for you?
November 30, 2021
When you go to an Orthopaedic doctor for foot and ankle care it is very likely you will be getting some sort of imaging done. When evaluating a patient, aside from the patient’s history and exam, an Orthopedic surgeon uses imaging to guide treatment. In most cases, doctors can tell a lot from basic plain films or radiographs (X-Rays). These tests help the doctor in their guidance with the next step for the patient.
The vast majority of patients can be treated without advanced imaging and use radiographs to treat them appropriately and successfully. Specifically in lower extremity orthopedics, it is important to get weight bearing X-Rays. These will help show the alignment of the leg, ankle, and foot, while guiding the doctor towards the process of how to treat the patient and what they may need to correct. In some cases, advanced imaging may be recommended to help determine the nature of the problem. These include: magnetic resonance imaging (MRI), computed tomography (CT), ultrasound and bone scans. Below are many of the imaging techniques used by foot and ankle specialist, Dr Adam Miller, to help determine the next step in his patient’s journey. Here is what you can expect.
X-Ray: The most common imaging technique. X-ray uses small amounts of radiation to detect the mineral in bone. This image is captured for the orthopaedist to view. They help detect fractures and more specifically the type of fracture. Fractures can have different characteristics based on the timing. This helps Dr. Miller determine if the fracture is healing and how old the fracture is. With these findings there are certain hallmarks to look for in determining what the fracture looks like. In some more rare diagnoses such as oncology or cancer, there are specific characteristics we look out for to make sure there is nothing abnormal going on that would be of concern. X-Rays are sometimes helpful to determine metal foreign bodies.

In orthopaedic foot and ankle care, X-Rays help evaluate the alignment of the patient’s bones. One can also determine the amount of chronic changes such as arthritis. These X-Rays are then used to set a plan with the patient. Follow up X-Rays subsequent visits are used to check on a surgery outcome or to check on healing of an injury. The time continuum of the X-Rays at each visit helps us know how the healing is going.
MRI: The second most common study is an MRI or Magnetic Resonance Imaging. No radiation is required. Instead, this uses magnetic fields to create detailed images on a focal part of the body. MRI’s give very detailed imaging of essentially everything: bone, soft tissue and can determine the difference between tendons, ligaments, bone, fluids, and solids. These are very helpful with subtle injuries but also soft tissue injuries that the X-Rays can’t pick up. For example, if you were to have the following: sprained ankle, cartilage injury, subtle bone injury such as a stress injury, or different changes of arthritis. All these injuries can be picked up on an MRI much more accurately. For example: an X-Ray may not be able to show a stress fracture for 2 weeks before any subtle changes occur. But on an MRI within a few days, it is over 95% accurate for a stress injury. These are often obtained to make a diagnosis or plan for a surgery.

CT: A CT Scan (Computed Tomography Scan) is a 3-D scan of bone and soft tissue which uses radiation instead of magnetic imaging. Orthopaedists use CT’s when they’re trying to see very fine bone detail. Certain bone specific diagnoses require a CT to see more bone detail than what an MRI can give you. A CT is also best used in cases where a patient already has metal in their body that limits the field of view on an MRI. Sometimes we use CT to determine healing and if a certain bone healed completely.

Ultrasound: An Ultrasound is a dynamic study. Unlike other imaging studies, the imaging is obtained in real time allowing the ultrasonographer to have the patient move and react to what they see. This allows us to check if anatomy is moving correctly and how structures look in different orientations. Usually ultrasound is performed when the patient is active in the office, and is used to look at anatomy while the patient is moving. It also allows us to look at different areas on the patient at one time. This can help to really see the movement of the anatomy such as a tendon or bones coming together. It is helpful to perform injections in certain joints that are difficult to identify skin deep. We use these for different steroid injections and other types of injections.

Bone scans are a group of studies using an injection in the body through a vein. This fluid spreads throughout the body and pools in active areas of the bone. How the fluid acts gives clues to various diagnoses. There are several uses in orthopaedics such as periostitis, stress fractures, inflammation, infection, and cancer.

If you think you may need imaging done do not wait, we are here to help! Dr. Miller is Beacon Orthopedics foot and ankle specialist and is available at several locations around the Cincinnati area. Contact us today for more information! Click here to learn more and schedule an appointment with Dr. Miller for your foot and ankle injuries.
Are your flat feet causing you pain?
October 26, 2021
Many people think they have flat feet, but how do you really know? Do you feel like you are having a lot of foot issues but you’re unsure of what to blame? Maybe the shape of your foot is part to blame for your pain. Here is how to tell if you have flat feet and learn about commonly related pain.
How to know you have flat feet:
Let’s first look at a few characteristics of a “planovalgus deformity” or flat foot for short. The initial evaluation for the leg should look at the alignment of the foot in a standing position. One of the most important factors in orthopaedic surgery is the alignment and mechanical access of your leg. This means that in neutral alignment the ankle and heel rest underneath the lower leg. If this alignment is off, that can be a reason why you have pain on one side of your foot. Imbalance in the leg adds excess stress to either side of the foot. This results in pain and structures working overtime to compensate.
Early on while evaluating a patient, Dr. Adam Miller wants to see the position and alignment of the leg. This allows him to narrow down the potential issues that the patient could be facing. There are specific characteristics to the shape of the foot that determine the foot alignment and position. One thing Dr. Miller looks for is if he can see the inside of their heel. If the inside of the heel is visible, this means that the foot is higher arched. If he is not able to see the inside of the heel, then their feet are either straight or displaying out to the outside which would be more of a traditional flat foot characteristic.
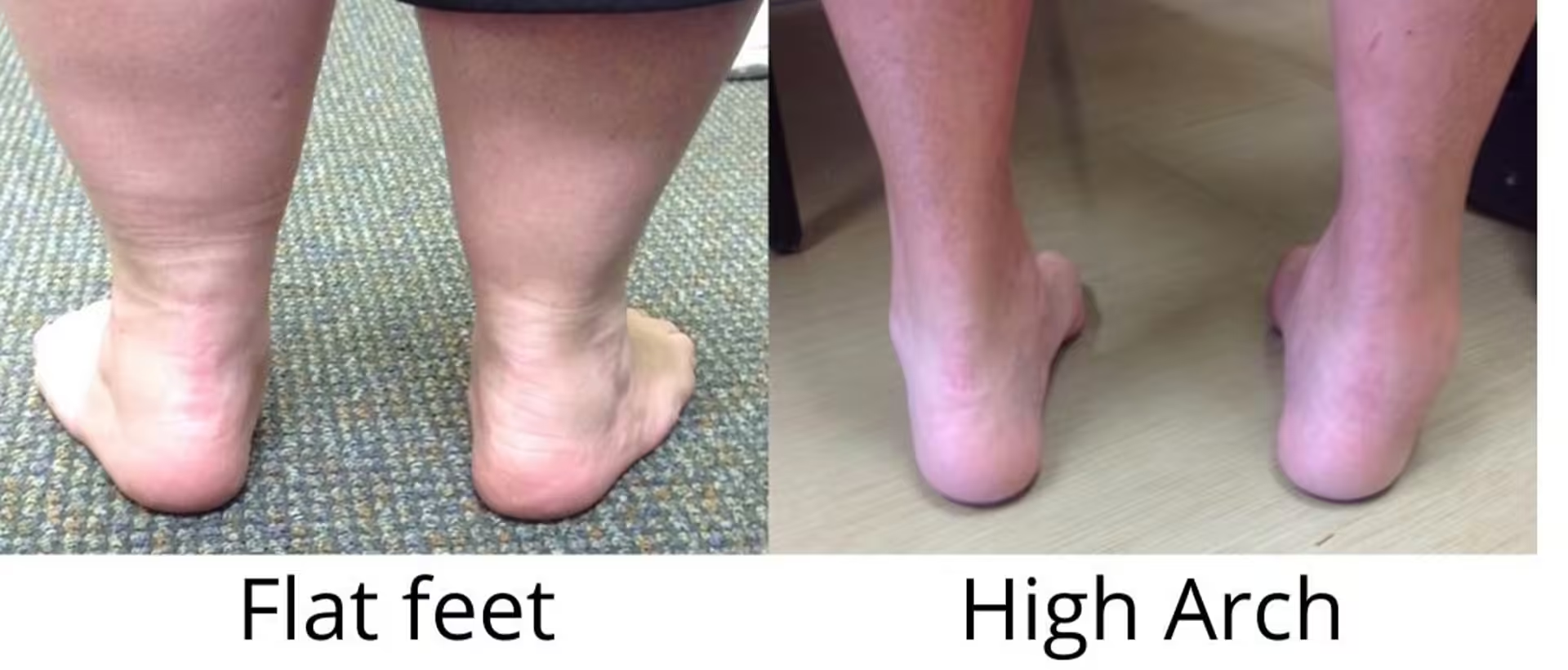
Next, he looks at them standing from the back side to assess how the heel lines up. This poses the question “Is the heel underneath their leg or is it to the outside?” If it is towards the inside, the patient is more of a high arched individual.
The last thing the doctor will look for is the “too many toes” sign. This means the patients foot rotates out externally or to the outside and a lot of the forefoot is showing even from behind. Here you can see this as well as the heel position in the flat foot.
All these assessments are general tests you can try right at home in front of your mirror! When you try it, stand parallel to the mirror, and let the feet relax at shoulder’s width apart. This will allow you to gauge the general characteristics of your foot. If you start to realize you are trending towards flat foot characteristics, this may be just the issue if you’re experiencing pain.
Common areas of pain with flat feet
There are a few beginning places to look when a patient is experiencing pain and they have some flatness or “valgus” alignment issues in their foot. This will trigger that the foot is the problem in relation to the alignment. The most common area of pain is on the inside of the ankle and foot. 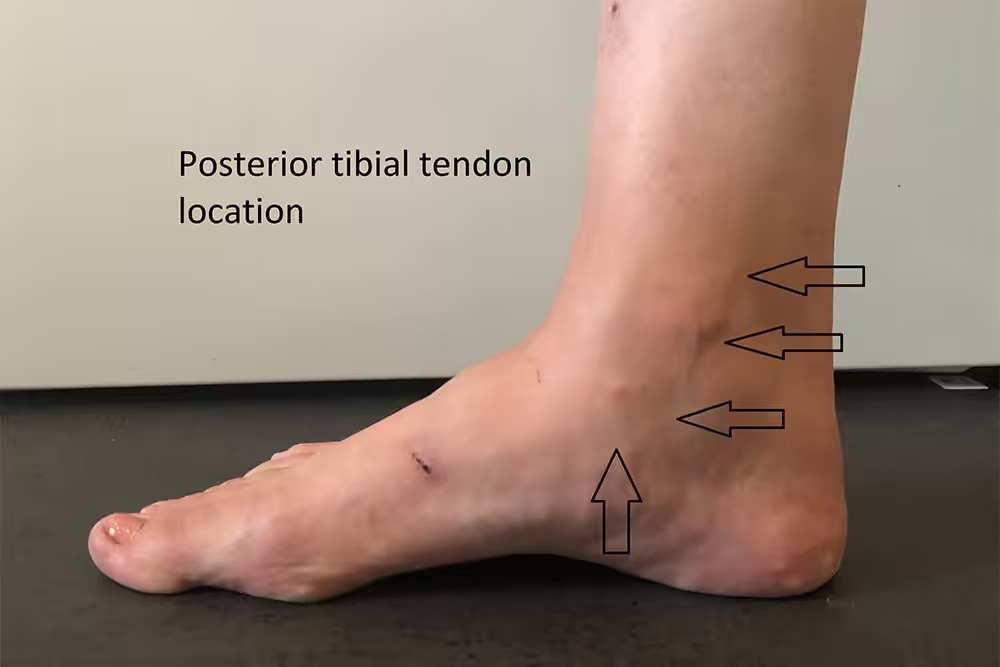
This pain can be isolated to the inside of your arch or be felt behind the ankle going up the lower leg. This is caused by the posterior tibial tendon on the side of your ankle that holds up the arch and controls the foot arch. This is a very large tendon (tendons are like ropes that attach muscles to bones to make your body move.) that essentially controls your arch. When the foot is flatter and sags to the inside, the posterior tibial tendon must “work harder” and is more susceptible to tearing, degenerating, and pain.
The second most common place of pain is on the outside of the foot, right underneath the ankle (fibula) bone which is what we call impingement.
Patients who have more severe flat feet develop this pain. Their foot starts to swing out from underneath their leg such that the heel bone starts to hit one of two ankle bones incorrectly. Instead of your heel bone being underneath your leg, it starts to impinge and hit your ankle bone (fibula). This can become very painful over time.
Another thing often painful for someone who is flat foot is when they go to stand on one foot and raise their heel off the ground. This single heel rise can recreate pain on the inside of the ankle. This maneuver activates the posterior tibial tendon and is common in flat foot related pain.
Many younger patients may have pain and prominence on the inside of the arch on their foot. This may be caused by accessory bones in that area where the posterior tibial tendon inserts. This focal area on the inside of your foot can then again become very painful. 
It is important to note that flat feet don’t always have to be painful. It is perfectly normal to have a flat foot. There is a bell curve of normal…. some people are high arched, some people are in the middle, and some people just have flat feet. We try to focus on the individuals experiencing pain. We can’t predict whether people are going to have pain with flat feet, nor can we do anything to prevent the foot from becoming flat. However, the shape may predispose someone to developing pain in certain areas. You can wear your choice of arch support, but this has never been proven to change the natural progression of your arch or alignment.

What can we do/ treatment:
Initially, when a patient first comes in with pain related to a planovalgus (flat foot), we always try to recreate the arch with a support device and make the foot as neutral as possible. Non-surgical treatment is always the best first option which is dependent on the severity of the patient’s pain and problem. If they are unable to walk, we usually will start with a boot. If the pain is mild or intermittent, then an insert in the shoe or a brace may be more appropriate. 
![]()
Depending on how the patient is tolerating the transition, we will try and wean them back to normal. Many times, improving flexibility and calf stretching is important, along with physical therapy. However, if these measures fail, we then start turning our attention to surgical intervention.
If you think you may have flat feet and are experiencing pain, we are here to help! Dr. Miller is Beacon Orthopedics foot and ankle specialist and is available at several locations around the Cincinnati area. Contact us today for more information! Click here to learn more and schedule an appointment with Dr. Miller for your foot and ankle injuries.
Fall Sports Injuries
September 28, 2021
School is back in session which means athletes are back on the field ready to kick off their Fall sports seasons! This time of year we start to see a spike in athlete injuries like football, soccer, and volleyball. So, what are some of the things to look for in potential injuries an athlete may endure? Here is how to know how severe the injury may be and when to seek care.
Contusion:
Just like anywhere else on the body, your foot may have a bruise or a contusion of the foot. What is a contusion? It is just that, a bruise on your bone. The most common occurrences we see is when a player gets kicked, stepped on, or cleated in the ankle, foot, or lower areas of the leg. Majority of athletes can continue playing their sports when having a contusion, however they may not be feeling 100%. Many of times the ability to play is due to the adrenaline rush that keeps the athlete going and not feeling the pain in the moment. After the game, when the athlete gets a break or time to rest then they start to realize that there may be a potential injury. One strategy we recommend before seeking care is to use the RICE method listed below.

Rest, rest, rest!
Ice is a good pain reliever and lowers inflammation.
Compression applied with ace helps with swelling while providing stability.
Elevate the injury to relieve swelling and limit the amount of bruising.
You must give the injury enough time. It is a battle of pressure and wanting to get back on the field, but what the body really needs is the adequate amount of time to rest up and heal. If the athlete is still experiencing pain and struggling to walk, it is time to seek a professional for care.
How to know if it is a contusion? With a contusion, the athlete can usually pinpoint the focal area that is causing pain. The foot may be showing signs of mild swelling but overall, the athlete can still put weight on the foot and wear a shoe.

What’s the next step? Getting an x-ray will show that the athlete is negative with a contusion. They will be put in a boot to let them simmer down and weight bare in the boot. Next, an evaluation will be taken in 1-2 weeks to ensure there’s no more concerning injury shown. In most cases, the athlete can extricate themselves from the boot in just a couple of weeks. If they are doing well walking in the boot with no pain after a few days, the boot will be removed, and they will be allowed to start walking on the field starting with low impact exercises, in hopes to return to playing shortly after.
More severe cases:
 When there is a more severe injury things become a bit more complicated. With athletes, these cases may be caused by someone falling on the leg, a pile up in football, or the athlete falls and rotates their ankle or foot. The athlete will have an immediate out from their game followed by trouble walking. Many players will come in under their own power likely needing crutch assistance. They are usually seen quickly after the injury because of the level of pain. The swelling is much more considerable and there is usually bruising involved (bleeding from the inside). These patients will need an x-ray to see if the damage is severe enough for a surgical repair. The x-ray shown is an example of a serious ligament and bony Lisfranc injury.
When there is a more severe injury things become a bit more complicated. With athletes, these cases may be caused by someone falling on the leg, a pile up in football, or the athlete falls and rotates their ankle or foot. The athlete will have an immediate out from their game followed by trouble walking. Many players will come in under their own power likely needing crutch assistance. They are usually seen quickly after the injury because of the level of pain. The swelling is much more considerable and there is usually bruising involved (bleeding from the inside). These patients will need an x-ray to see if the damage is severe enough for a surgical repair. The x-ray shown is an example of a serious ligament and bony Lisfranc injury.
 What injuries specifically? Usually, a fracture or ligament injury will fall into this category. Regarding the ankle, many rotational injuries can result in an ankle fracture (Is it sprained or broken blog). If the athlete experiences a lot of swelling in the ankle and the inability to walk it is very important to get an x-ray and check to make sure there is no fracture or the need for surgery.
What injuries specifically? Usually, a fracture or ligament injury will fall into this category. Regarding the ankle, many rotational injuries can result in an ankle fracture (Is it sprained or broken blog). If the athlete experiences a lot of swelling in the ankle and the inability to walk it is very important to get an x-ray and check to make sure there is no fracture or the need for surgery.
Regarding the foot, the most common and concerning injury is a Lisfranc injury. This is an injury that goes back to a general in Napoleon’s army that noticed people were twisting their feet in stirrups and these injuries were devastating often leading to amputation. The concern here is the injury from twisting is severe and most come on strong directly through the foot, which we would call an axile loading type injury.This occurs when you’re standing on the ball of your foot and a load goes straight through the long axis of the foot (as seen in the picture). These injuries may be severe and will likely require surgery.
 What to look for with these injuries and when to be concerned it’s a Lisfranc injury? Bruising on the bottom of the foot is the best tell-tale sign (as seen in the photo). If the foot is at all twisted the athlete will be experiencing severe pain in the middle of the foot. The injury will be very painful in the first few days to a week but, if the athlete doesn’t seek care, sometimes the pain will diminish, and they may not be as concerned about the injury. It is important to get these injuries checked out because that slight sign of improvement can give a false sense of optimism or hope that the foot will heal, which may lead to collapse and arthritis down the road.
What to look for with these injuries and when to be concerned it’s a Lisfranc injury? Bruising on the bottom of the foot is the best tell-tale sign (as seen in the photo). If the foot is at all twisted the athlete will be experiencing severe pain in the middle of the foot. The injury will be very painful in the first few days to a week but, if the athlete doesn’t seek care, sometimes the pain will diminish, and they may not be as concerned about the injury. It is important to get these injuries checked out because that slight sign of improvement can give a false sense of optimism or hope that the foot will heal, which may lead to collapse and arthritis down the road.
Rolling of the ankle due to un-even ground:
 When an athlete sprains their ankle, if there is the ability to get a trainer to tape it or wear a brace allowing the athlete to bear weight and make some of the basic maneuvers, then they can keep playing. If they are unable to keep playing, the initial steps are short term immobilization: usually being able to walk in a boot or brace. If the pain is too significant, the player would start in the boot and transfer over to a brace as the time goes on. Usually, you don’t want to wear the boot for much more than a week. If this seems necessary, it usually says that there is more going on and a specialist would want to look further into the injury.
When an athlete sprains their ankle, if there is the ability to get a trainer to tape it or wear a brace allowing the athlete to bear weight and make some of the basic maneuvers, then they can keep playing. If they are unable to keep playing, the initial steps are short term immobilization: usually being able to walk in a boot or brace. If the pain is too significant, the player would start in the boot and transfer over to a brace as the time goes on. Usually, you don’t want to wear the boot for much more than a week. If this seems necessary, it usually says that there is more going on and a specialist would want to look further into the injury.
After transitioning into the brace, under the guidance of a physical therapist or an athletic trainer, one can begin rehabilitation of the ankle. Generally, a brace and therapy allow people to avoid surgery and recover 85% of the time from a significant ankle sprain. With an ankle sprain injury, the RICE method (mentioned above) is super important to help your injury with healing. If it seems as if your sprain is not improving over the first few weeks or you may be having difficulty walking and returning to the sport, this would be the time to come in and schedule an appointment to get the injury looked at.
If you’re an athlete seeking for care do not wait, we are here to help! Dr. Miller is Beacon Orthopedics foot and ankle specialist and is available at several locations around the Cincinnati area. Contact us today for more information! Click here to learn more and schedule an appointment with Dr. Miller for your foot and ankle injuries.
Does Your Foot Hurt Here?: The Heel
July 1, 2021
Pain in the heel is incredibly common and a vast majority will typically fall into a few different categories. These pains will most likely develop over time, however few will present seemingly out of the blue. There are several nonsurgical ways to treat these problems to better the pain. In fact, it is less common to need surgery in the first place. Let’s get into a few of the most common and treatable types of heel pain.
Achilles Tendon
The Achilles tendon is the longest and strongest tendon in your body. Given its strength, the tendon endures a lot of force. Traditionally over several months and years, there can be scar tissue that builds up with wear and tear that occurs to the tendon. Sometimes even bone spurs will form insidiously along the back of the heel imbedded in the tendon.


 Symptoms: The body’s reaction to these processes results in more scar tissue and even more bone spurs. Those changes can be painful and it is possible to notice thickening pressure in the back of your shoe, focal prominence, and pain with walking and motion in the heel. Located directly in the back of the heel, the pain does not typically radiate on the bottom; however, pain may be present on the sides.
Symptoms: The body’s reaction to these processes results in more scar tissue and even more bone spurs. Those changes can be painful and it is possible to notice thickening pressure in the back of your shoe, focal prominence, and pain with walking and motion in the heel. Located directly in the back of the heel, the pain does not typically radiate on the bottom; however, pain may be present on the sides.
Treatment: In the beginning, a common solution is to get a heel cup or lift to take the tension off the heel (think high heeled shoe!) This will relax the tendon and allow it to heal and calm down. There are also many topical anti-inflammatories that are found over the counter that are often recommended. Once the treatment starts relieving swelling and feeling better, its best to start some light stretching. This focuses on the calf and hamstrings. If the pain is not feeling any better after a few weeks, then it may be necessary to get an x-ray and evaluation with Dr. Miller. There are several options depending on the severity and activity level that are likely beneficial.
Plantar Fasciitis
Plantar Fasciitis is pain attributed to the bottom of your heel and is one of the most common things that an orthopedic surgeon will see. Plantar fascia is a cord of tissue from the bottom of your heel that goes to your toes. It is made up of collagen tissue and helps support the arch of the foot. Think of this structure as the bowstring to the arch of the foot. Although there are several theories as to why this occurs (including tightness and contracture in the legs), there still isn’t a great understanding of what causes plantar fascia and is often treated in many different methods.
Symptoms: Often times, people will experience this pain when first getting up from sitting or first thing in the morning. This pain is located directly at the bottom of the heel pad closer to the arch and may be manageable during different parts of the day. Typically, the pain tends to improve as the day goes on, but not always. Severe cases can last constantly.
Treatment: Patients suffering from plantar fasciitis are urged to try several modalities at once because the remedy might be different from one patient to another. The first area to target is flexibility, a key to recover from this problem. Try to focus on the calf stretching initially. The more flexible the ankle is, the less stress there is on the soft tissue. In this case, a heel cup or full-length shoe insert is a good idea because it will redistribute the weight the heel is bearing so the force can be spread throughout the foot and the arch. Another remedy to relieve the pain is a night splint that will target the flexibility while the body is sleeping. This will further help the morning pain in the heel. If these modalities are not helping in recovery, then it is appropriate to get an evaluation with Dr. Miller and make sure it is actually plantar fasciitis. Other options for recovery include an injection or other non-surgical treatments such as shockwave therapy or biological type treatments such as platelet injections. These should be discussed as needed at your evaluation.
Stress Fracture
A common type of bone injury to the foot or heel is a stress fracture. Repetitive activity is often associated with this type of injury. Often young kids play sports all weekend long and end up with unremitting pain and difficulty walking. People who stand on their feet several hours can suffer bone injury. Runners classically suffer from this type of problem. Stress fractures can be caused from many different activities or more aggressive force on the heel. True fractures of the calcaneus are usually from a fall from the height of 4-5 feet or more. Those accidents may be traumatic with lots of swelling and bruising along with it.
Symptoms: Stress and bone pain in the heel is a generalized pain all around the heel. It is often not just on one side of the bone. It comes with continuous pain and does not resolve as well as the day goes on.
Treatment: Any traumatic fall from a significant height should be evaluated immediately. At that point, the foot should be non-weight-bearing prior to x-ray evaluation. If there was no associated trauma, boot therapy is often enough to begin treatment. Timing and duration are usually best assessed in the office with Dr. Miller.
Are You Suffering From Heel Pain?
Dr. Miller is available at several locations around the Cincinnati area with Beacon Orthopaedics to assess your lower extremity. Contact us today for more information! Click here to learn more and schedule an appointment with Dr. Miller for your foot and ankle problem.
How to Decide if That Foot Pain is a Fracture
May 25, 2021
When trying to assess your new foot pain, it’s important to keep note of even the most minor injuries as they can become something more if not protected appropriately.
Whether you dropped a jar on your foot or got stepped on in a game of soccer, don’t dismiss the pain. Sometimes the pain can come on slowly over time; it’s important to know when to get an evaluation.
Direct Impact Injuries and Contusions
In most cases, an appropriate measure for the first couple of days is to assess if the injury is too painful to continue activities. If mild, walk or play through the pain temporarily. However, if you continue to feel pain that is either staying the same or getting worse, you may have developed a bone bruise, or contusion of the foot. This means there is enough injury to the bone without fracture to compromise the integrity of the bone. Your body responds with pain to try and avoid using this area of your foot. The most common place where we see these happen is the metatarsals (pictured here). If these smaller bones are bruised to the point where the integrity is challenged, the continuation of playing or walking can make it prone to a delayed injury or even a delayed fracture.
Make sure to be mindful that the pain is rapidly improving over time. If the injury is not improving as it should, you may find yourself requiring oral medications such as Tylenol or anti-inflammatories to get through the day. It’s at that point where it’s worthwhile to get an evaluation so you don’t sustain an injury that could have been properly prevented.
Stress Fractures

Stress fractures or stress reactions are injuries typically found on the top of the foot in the metatarsal area (shown above). While they can occur in almost any bone, these are the most common. These seemingly trivial injuries can occur over time by simply running on a new trail or through new repetitive movements. This change in activity triggers stress and that repetition can further cause additional stress fracture scenarios. The most common areas we see these fractures are the second through fourth (see image to the right) metatarsal. The first metatarsal is too big and too strong to sustain one of these injuries. If you are not seeing improvement over a few days, or weeks’ time, then an evaluation is highly recommended. In these cases, x-rays are important to make sure that a fracture is not developing. If the bone has been injured enough, then proper equipment is required to help in the healing process. Whether that equipment be a sandal or a shoe adjustment, it is appropriate to make sure they minimize and improve the state of your forefoot before you are ready to get back to activity. The proper equipment is important. A boot may be required instead of a sandal. This is dependent on the individual’s radiographs and the patient’s history. In addition, how long you must wear the device and how much activity during a day are important variables to ask when being evaluated. Ideally, you want to see 1-2 weeks of no pain before you start to ramp up the activities again while being off pain medication completely. Dr. Miller will give you explicit advice how make these injuries better.
Twisting and Midfoot Sprains
What is a foot sprain? Just like an ankle sprain, the ligaments that connect bones in your foot can be injured. When those connections are partially injured or ruptured, a foot sprain can be a significant injury. How do you know if your foot is sprained? Many times, we see injuries where the foot will have an awkward landing underneath your ankle. These injuries can be painful enough making it difficult to walk or a moderate pain that simply won’t go away. When that happens, certain ligaments in the middle of your foot (Lisfranc ligament, see image to the left) can get injured, which sometimes require surgery to treat or immobilization. These injuries are characterized by pain on the top of the foot just closer to the ankle than the metatarsals. Sometimes these injuries may also seem trivial if you land the incorrect way, either with your foot falling underneath, or an axial twist of the foot. Both scenarios can result with pain in the middle of your foot. These injuries cause pain on the top of the foot in the middle of the arch. (Black arrow) They also necessitate a prompt evaluation with Dr. Miller to know the severity of the injury and appropriate treatment. Often times they do not get better on their own no matter the grade or level of injury unless immobilized with a boot.
Why are evaluations important?

A proper orthopaedic evaluation consists of a hands-on thorough exam, appropriate x-rays taken with good technique, and possibly advanced imaging studies obtained promptly. At Beacon, we have the capability of obtaining rapid imaging studies and we take pride in offering prompt evaluations. Carefully evaluating these injuries are always important because you want to avoid making an injury worse and be able to recover as fast as possible. Neglecting the injury will often delay recovery. For example, a stress fracture may become a complete fracture. They can move, displace, and require surgery or heal very slowly because of continued use. Without an evaluation, it is very difficult to know if you need surgery or if it’s amenable to boot type non-surgical therapy without really being seen. It’s important not to hold off and come in sooner rather than later because these injuries often necessitate several weeks off. Midfoot sprains, or Lisfranc injury, can be very serious if not evaluated within reasonable time. Often if a midfoot sprain is severe and left untreated, the foot can collapse, change shape, and arthritis eventually ensues with chronic pain.
Do you have nagging foot pain?
Don’t wait, get an evaluation today! Dr. Miller is available at several locations around the Cincinnati area with Beacon Orthopaedics. Contact us today for more information! Click here to learn more and schedule an appointment with Dr. Miller for foot and ankle injuries.
Spring is here, prep for sports this year!
April 5, 2021
Baseball is upon us, local sports teams are finally practicing and playing outside, and runners are out in full force. There are a few things to be mindful of to prevent injury while engaging in high intensity sports. Whether it be a baseball player or track star- long jumper, new injuries tend to arise within the first few weeks into the season. These injuries are due to new forces upon lower extremities that the body is not used to. Common injuries from these new forces could include stress fracture, ankle sprain, ankle or foot buckling, or more serious injuries that could need surgery. You may be asking yourself: “How do I prepare for sports this year?” Let’s go over a few crucial tips to keep you moving and out of the orthopedic clinic.
Warming Up
It is always important to warm up your muscles before use. This will go a long way to preventing injury. Doing so provides oxygen to the local tissues. Stretch before your warm-ups and focus on calf muscles performing stretching several times a day. The more flexibility you have allows the leg and foot to tolerate more strenuous activity. A lack of flexibility leads to muscle strain or undue forces that can injure the foot and ankle. Keep in mind: you are a year older than last Spring! It takes longer to warm up with age and conditioning becomes more important each year.
Proper Equipment
A commonly asked question is “what shoes are best?”. The best answer is finding a shoe that properly fits you. Studies have shown more people buy too small a shoe. Improper sizing leads to pressure, blisters and awkward landings that can be hurtful overtime. Try buying a cleat with more room to fit an insert for added support. Runners should obtain a shoe that compliments your foot shape. For example, flat footed people should wear a shoe with more medial or inside support.
How should I treat a common sports injury immediately after it happens?
Orthopedic Foot and Ankle Specialist, Dr. Miller, suggests asking yourself first: “Can I continue playing or do I need to walk away?” An honest answer to this question allows your body to recover from injury instead of prolonging a recovery. In addition, some serious injuries can be subtle, so make sure to look for swelling and bruising. If you can’t run, try walking! Some injuries may bother you, but not enough to act immediately. In this case, give the injury one to two weeks of modified activity and allow your body to naturally heal. If time passes and you have not improved, you can’t walk or put weight on the foot, it is time for an orthopedic evaluation.
Is it risky to play through injury? 
Almost always the answer to this question is yes! Pain is the body’s natural feedback loop to your brain saying stop. One of the most difficult aspects in helping people heal is balancing the return to activity with the time the body needs to heal. Going back too early commonly prolongs an injury or may lead to necessary intervention. It is super important to listen to your body and know when you are just doing too much.
How can I treat an injury on my own initially?
If you can walk with modest pain, then seeing if the injury improves in 1-2 weeks is warranted. During that time use the RICE method:
Rest, rest, rest.
ICE is a good pain reliever and found in studies to be a mild analgesic. Not only does this serve as pain relief, but it lowers inflammation as well.
Apply compression with Ace. Ace will help with swelling while providing stability.
Elevate. Elevate the injury to relieve swelling and limit bruising.
We’re Here for You
This Spring remember to treat your body right and prevent injury. Condition the body prior to activity by warming up and performing adequate stretching. Prevention of injury also comes with the proper equipment. Get fitted for the right cleats and shoes. Don’t play through an injury and remember allowing the body to recover after vigorous activity is important.
Suffering from a foot and ankle injury? Worried about a nagging pain prior to a race? If someone you know is needing foot and ankle care, Dr. Miller is Beacon Orthopedics foot and ankle specialist and is available at several locations around the Cincinnati area. Contact us today for more information! Click here to learn more and schedule an appointment with Dr. Miller for foot and ankle injuries.
Child Injuries and Injury Prevention
August 27, 2020
We are all facing more time at home—and therefore the risk of home injury. While you would normally be gearing up for kid activities or sports, now you are forced to entertain at home…yikes. Child injury prevention, and home safety, is even more difficult with no break in sight. You may be shouting, “Get me out of here!” Here are a few reminders and what kinds of orthopedic foot and ankle injuries can occur while staying at home.
For the young ones, it is often all hands on deck. Constant monitoring is needed. Falls from standing can occur, but often, injuries requiring medical evaluation are from a height. Stairs are particularly dangerous while everyone is forced into be in the house. Stairs are one of the most common mechanisms of injury I see for ankle fractures in adults. Here are some tips for those parents:
- Use baby gates for age appropriate children

- Do no leave object on the stairs
- Make sure there is adequate lighting for ascending and descending stairs
Kids are active at home now more than ever. Trampolines are increasingly common to pass time. In 2018, 30,000 injuries were treated, and this is likely to increase. In the leg, ankle sprains are one of the most common injuries reported from trampolines, but we have seen fractures and other injuries requiring surgery, too. Safe usage is meant to curtail these injuries:
- One child at a time is safest
- Child must be at least 6 years old
- Ensure equipment is working and maintained
- Adult supervision is recommended
Playground equipment is also a hot spot for children injuries. Falls are the most common and severe injury seen by medical personnel. Slides also are precarious when an adult takes a child with them. The leg of the child can get caught underneath the adult, fracturing the tibia.
- Lead children to age appropriate equipment
- Adult supervision is recommended
- Appropriate padding underneath the equipment should be present
Child injuries can be assessed by us at Beacon Orthopaedics via in-person clinical evaluations and telehealth online visits. Appointments can be made online or by phone at 513-354-3700. To stay in touch with updates and information, follow us on Facebook, Instagram, Twitter. We are ready to help.
Come to Beacon Orthopaedics & Sports Medicine
If you have a foot or ankle injury, come to Beacon Orthopaedics. We specialize in all things orthopedics, from hip and knee injuries to spine surgery. Contact us today for more information! Click here to schedule an appointment with Dr. Miller for foot and ankle injuries.
Top Doctors 2020 at Beacon
January 15, 2020
Each year, physicians are selected by their peers in a survey, asking them which physicians they would turn to for their own personal care. Beacon doctors – 25 Tri-State physicians – were named to Cincinnati Magazine’s Top Docs List of 2020. We are very proud of all of our physicians and thank the medical community for their recommendations. Click on any of the physician’s names below to view their personal profile page, orthopedic specialty and discover why their peers view them as top doctors in the Cincinnati region.
You can schedule an appointment with our Board Certified and Fellowship Trained physicians online or by phone 24/7 with no referral necessary. Beacon has nine convenient locations, evening and weekend appointments and urgent orthopedic care clinics so that patients can get the care they need quickly.
Top Docs 2020:
Foot & Ankle Surgery
Hand Surgery
Orthopaedics Surgery
Pain Medicine
Physical Medicine & Rehabilitation
Spine Surgery
Sports Medicine
You can schedule with our physicians 24/7/365 online or by phone at (513)-354-3700.
Pain Medication Safety
November 5, 2018
SAFE Use, Storage, and Disposal of Prescription Opioid Medicines from the American Academy of Orthopaedic Surgeons.
Unfortunately, prescription drug abuse is a serious public health issue, widely referred to as an “epidemic” by public policymakers. Opioids are prescribed for short-term pain reduction, but can be extremely dangerous if used improperly.
Safe Use of Your Prescription:
Please be aware that improper use of prescription pain medication is a leading cause of accidental death. Please keep the below suggestions in mind to ensure the proper use of your prescription.
- Combining opioids with alcohol or other drugs increases the risk of death
- Take medications only as prescribed.
- Never take more than instructed
- Never take somebody else’s medicine
- Never give or sell your medicine to someone else
- Combining opioids with medicines used to calm anxiety can result in overdose
- Using opioids for something other than pain (anxiety, sleep, fear of pain, to feel good) can create a harmful dependence/addiction
Storing Your Prescription Safely:
Unused medicines in your home risk being used inappropriately.
Pain relievers are a leading cause of serious poisoning of children and pets when they are left where others can get them
Hide or lock up opioid medications to avoid access by family, friends, or houseguests
Keep prescription medications in their original packaging so it is clear for whom the medications were prescribed and to save the directions for appropriate use
Safe Disposal:
Place all unused prescription opioids in the proper disposal unit at your local pharmacy or police station. There are dozens in Greater Cincinnati and the surrounding areas.
To search for a registered disposal site convenient for you, please click here.
In the rare case no medicine take-back facilities are available within your area, you can flush your unused medication down the toilet or follow these simple steps to dispose of most medicines in the household trash:
- Mix medicines (do NOT crush tablets or capsules) with an unpalatable substance such as used coffee grounds or kitty litter;
- Place the mixture in a container such as a sealed plastic bag; and
- Throw the container in your household trash.
- Before throwing out your empty pill bottle or other empty medicine packaging, please be sure to scratch out all of the information on the label to make it unreadable.
Is Ankle Replacement the Solution for You?
September 23, 2017
What is Total Ankle Arthroplasty (Ankle Replacement)?
Ankle replacement surgery serves to treat a patient with severe arthritis of the ankle by resurfacing the bone surfaces at the ankle joint. Metal components articulate with a plastic component to allow for pain relief and range of motion. Recent research has shown improved outcomes and survival rates for ankle replacements as a viable solution for severe ankle arthritis, and several patients at Beacon have taken advantage of this option with our team. Let’s go over some of the basic information you need to know about this exciting surgical treatment.
What is ankle arthritis?
 The ankle joint is a complex structure that includes three bones: the tibia (the major leg bone), the fibula (the smaller leg bone), and the talus. These bones interact to allow for motion at the ankle joint. Ankle arthritis is a condition in which the ankle joint cartilage wears out. Patients experience pain, loss of motion, swelling, and disability. There are several causes of ankle arthritis:
The ankle joint is a complex structure that includes three bones: the tibia (the major leg bone), the fibula (the smaller leg bone), and the talus. These bones interact to allow for motion at the ankle joint. Ankle arthritis is a condition in which the ankle joint cartilage wears out. Patients experience pain, loss of motion, swelling, and disability. There are several causes of ankle arthritis:
- Previous ankle trauma or fracture
- Ankle instability, severe ankle sprains over time
- Inflammatory arthritis (e.g. Rheumatoid)
- Osteoarthritis
- Other causes of arthritis such as gout or hemophilia.
What can be done to treat my ankle arthritis without surgery?
Nonsurgical treatment primarily consists of bracing and supporting the ankle to minimize painful motion. There are a variety of braces that can be used based upon the individual. Anti-inflammatory medicines are helpful for an acute exacerbation. Injection with corticosteroids on a limited basis may result in temporary relief of symptoms for pain. Although difficult, weight loss decreases the stress placed on the painful joint and typically relieves some pain.
If nonsurgical treatment fails, what can be expected with surgery?
Surgical options depend on the severity of the pain, amount of cartilage damage, and patient’s occupation, age, weight, and activity level. Early arthritis may benefit from an isolated removal of large bone spurs if present, with or without arthroscopy. The majority of ankle arthritis is treated by one of two methods: ankle fusion or ankle replacement. This is a complicated surgery that requires an orthopaedic surgeon’s background and experience in ankle replacement. The risks and benefits of each treatment can be complicated and are better suited for a full discussion with our team after a full clinical and radiographic evaluation.
What happens after surgery and how long will this affect my walking?
Ankle replacement surgery can be performed as an outpatient or an overnight stay at a hospital. A nerve block will help control pain during and after surgery. The leg would be protected in a splint until seen in the office 8-10 days later. A boot is used as a cast until seen 6 weeks after surgery. There is a period of no weight bearing initially after surgery to allow the bones to heal to the implants. Recovery usually occurs progressively over a six-month period.
Appointments can be made with Beacon’s foot & ankle specialist Dr. Adam G. Miller by calling (513)-354-3700 or booking online here.
Recovery Guide to Foot & Ankle Surgery
September 12, 2017
We are glad that you have chosen Dr. Miller for your foot and ankle surgery. Our goal is to make this experience as pleasant as possible for you. If you have any questions about your hospital stay, rehabilitation or recovery period, please contact Dr. Miller’s office for more information specific to your surgery.
Please click here to download the full informational PDF guide.
Low Vitamin D: Are Your Bones At Risk?
August 3, 2017
The Need for Vitamin “D”:
Vitamin D has been a hot button topic for years now. Why is it so important? Why do so many people have low levels and what are the implications of that?

The more we learn, it has become apparent the importance of this metabolite. Low “D” has been implicated in conditions such as rickets and osteoporosis. In fact, milk and other products were mandated fortification with vitamin D in the 1930’s due to rickets and the associated bone malformations observed in children. Besides consumption of dairy and now some orange juice, some fish obtain high levels of the vitamin.
The requirement of vitamin D in the diet comes from the decreased sun exposure that nearly all of us see. Whether you blame increased work of adults or video games in children, less outside activity is prevalent. In addition, dermatology places strong emphasis now on protection from skin cancers and melanoma through the use of sun block. The prevention of ultraviolet sun exposure to skin also prevents the activation of the metabolite.

Can Low “D” Cause Injury?
Beyond rickets (which is rare today with fortified products) and osteoporosis, vitamin D is associated with increased chance of injury. Recently a common fracture to the 5th metatarsal called a Jones fracture was recently found to be five times more likely in patients with low levels of “D”. There is also a suggestion that “bone edema” or bruising of bones is associated with low vitamin D levels. This suggests that elevating a low level of the metabolite may prevent some of these fractures. Therefore replenishment has been suggested to be appropriate is most cases if detected.
A normal vitamin D has been determined to be above 30ng/mL. Low vitamin D is highly prevalent in latitudes above 30 degrees (North of Jacksonville, Florida). So, chances are you have low levels! Before every surgery involving bone, I check a patient’s vitamin D level to ensure there is a minimal chance this will effect outcomes. Next time your doctor requests blood work, it may be worth checking…
For more information or a personal evaluation, please visit our website. Appointments can be made with Dr. Adam G. Miller by calling (513)-354-3700 or booking online here. If you are not following Dr. Adam G. Miller on social media, you can do so on Facebook or Twitter for: updates and comments on cutting edge treatments, discussion of various injuries, and sport/athlete issues.
Big Toe and Foot Pain – New Option You Need to Know
May 18, 2017
The Big Toe Pain Game Changer
Big toe pain can come in many varieties. One of the most common causes is arthritis in the toe at the metatarsophalangeal (MP) joint called “Hallux Rigidus”. This joint is an area of high stress. Pain is more common in women and a common site for arthritis in the foot. For years patients have dealt with pain in their big toe and been given few options. These include: antiinflammatories, shoe changes, activity modification, injections, and possibly surgery.
Many patients fear surgery when hearing that the surgical solution is a fusion of the joint. This requires the bones to grow together and involves placing metal screws and/or a plate in the toe for stabilization. Other options may not reliably take pain away.
A new product call Cartiva has been recently approved by the FDA. It is backed by research and years of use in Europe. This is essentially an implant placed in the big toe to prevent the grinding of the MP joint. Symptom relief in selected patients has been similar to fusion patients in a recent study. See the recent story by NBC Nightly News below.

The Cartiva implant is made of a similar material to a soft contact lens. The success rate is vastly improved to previous implants. And if the implants fails, a salvage fusion is still possible. Previous implants did not allow this.
Investigation into other uses for the implant material are already underway. This includes knee and hand treatment options.
Not all patients are appropriate for this new implant. However, in the right patient this can keep you going with minimal down time or motion loss. The implant is appropriate for all ages with big toe arthritis. To find out more about this exciting option, call us today for a full consultation or click here to schedule an appointment with Dr. Adam Miller.
For more information or a personal evaluation, please visit our website. Appointments can be made with Dr. Adam G. Miller by calling (513)-354-3700 or booking online here. If you are not following Dr. Adam G. Miller on social media, you can do so on Facebook or Twitter for: updates and comments on cutting edge treatments, discussion of various injuries, and sport/athlete issues.
Spring Sports Introduce New Ankle Injuries
March 21, 2017
What you need to know


Sun and warmth are just around the corner and that means high school and club sports are gearing up. Because these sports are outdoors on a field and often uneven terrain, the ankle is particularly susceptible to injury.
“Basketball and football are the sports we think of commonly to sprain an ankle, but with year round play and early spring competition we are seeing these injuries more consistently,” says Adam G. Miller, M.D., Orthopaedic Surgeon and Foot and Ankle Specialist with Beacon Orthopaedics and Sports Medicine.
Baseball, soccer, track are often played on fields that have undulations after the winter. These unsuspecting “landmines” can lead to a serious injury.
And sometimes serious injuries can go unnoticed. Miller cautions: “A rolled ankle may be the tip of the iceberg for the patient. It’s important to assess the entire lower extremity to ensure this doesn’t become a chronic issue.”
Here are some tips for ankle injuries:
- Initial protection is needed. Immediately after the ankle injury, apply ice and compression to the leg pain. Protection and rest is advisable until one knows the severity of the injury.
- Need to walk before you can run. After an injury if you can’t put weight on the leg to walk, it is advisable to make an appointment with a medical professional. This can be a sign of a complete ligament tear or subtle fracture.
- Beware of the plateau. If you are successfully improving following an ankle injury but then notice your recovery stops, don’t settle for partial relief. Chronic pain can be a sign of worsening injury such as a high ankle sprain, peroneal tendon tear or cartilage damage with osteochondral defect and should be evaluated.
- Learn from the past. While each new injury can recover similarly to previous ankle sprains, a history of multiple injuries can predispose a patient to more pain and instability that can be difficult to self-treat. A long history of ankle issues should trigger an office visit.
Bottom line: beware of the unsuspecting ankle injury that masquerades as a minor ankle “roll” and seek medical attention promptly.
For more information or a personal evaluation, please visit our website. Appointments can be made with Dr. Adam G. Miller by calling (513)-354-3700 or booking online here. If you are not following Dr. Adam G. Miller on social media, you can do so on Facebook or Twitter for: updates and comments on cutting edge treatments, discussion of various injuries, and sport/athlete issues.
Tips and Tricks for Common Injuries
March 21, 2016
As an orthopaedic foot and ankle specialist, I see two very common sources of pain: ankle sprains and general heel discomfort. While I definitely recommending scheduling with me, there are a few actions that can be taken to reduce pain or treat common injuries. If your pain persists or increases, please give me a call, or feel free to book an appointment with me online, in real time.
How to treat an Ankle Sprain
- Arrest play or activity to prevent further damage.
- Apply compression and ice to the ankle and injured area.
- Allow for rest time and during this elevate the extremity.
- If pain continues to worsen or you cannot walk, seek Orthopaedic consultation and call us 513-354-3700 or book online for a full evaluation.
How to improve new Heel pain
- Modify your activity most likely causing the pain (e.g., distance you are running, stride you are taking, etc.).
- Develop a stretching regimen to warm up your legs, and try working it into your daily routine.
- Use supportive shoes such as tennis shoes or running shoes, and consider using a prefabricated orthotic for customized support.
- Rest and give the injury time to heal and improve prior to reintroducing activities again.
- Try an anti-inflammatory for pain relief as long as this is not contraindicated by your medical doctor. Check with them prior to usage if unsure.
- If pain continues to worsen or you cannot walk, seek Orthopaedic consultation and call us 513-354-3700 or book online for a full evaluation.
About Dr. Adam Miller:
Dr. Adam Miller specializes in foot and ankle pathology, treating all types of problems in the lower extremity. It is his goal to relate to the overall health and orthopaedic function of each patient, and to provide them with comprehensive, personalized care. Dr. Miller currently sees patients at Beacon’s Summit Woods (Sharonville), Northern Kentucky (Erlanger), and West locations.
Foot & Ankle Injuries from Adam Miller, MD
October 26, 2015
Learn More About Foot & Ankle from Dr. Adam Miller:
Doctor Adam Miller, M.D. is one of the leading foot and ankle surgeons at Beacon Orthopaedics and Sports Medicine. As an active part of the American Orthopaedic Foot and Ankle Society (AOFAS) and FootCareMD, Dr. Miller had the opportunity to contribute his insights and experiences to a recently published article. Please click here to read the full article from the AOFAS and FootCareMD.
Dr. Adam Miller and other contributing experts in the field provided insight specifically designed for patients. These insights can also benefit the family members or parents of someone suffering from an ankle of foot related injury. Proper care for lower extremity injuries is important, and knowing how to avoid future complications is a big part of that. The collaboration of researchers and practitioners combined with the intention of providing patients and family members alike with an opportunity to learn about proper injury care.
If you have any additional questions, or if you would like to schedule an appointment with Dr. Miller, please give Beacon Orthopaedics a call at (513) 354-3700, or schedule online in real time by clicking here.
Dr. Miller, BioEngineering Advisor on Osteochondral Repairs Capstone
October 26, 2015
One of the doctors at Beacon Orthopaedics and Sports Medicine is partnering with undergraduates to improve osteochondral repairs in unstable joints. Dr. Adam Miller, MD is an orthopaedic surgeon serving the Cincinnati and Northern Kentucky area. Since Dr. Miller focuses on foot and ankle injuries, he is able to serve as an advisor to an ambitious group of bio-engineering college students.
University of Maryland’s Fischell Department of Bioengineering (BioE) touted sixteen impressive capstone projects. Dr. Miller’s team of students designed a customizable 3D tissue-engineering scaffold for specific applications.
 With his guidance, the students’ 2014 Senior Capstone project undertook an ambitious to a challenging problem. They were able to design a customizable three-dimensional tissue-engineering scaffold. Their scaffold supports full thickness osteochondral repairs in joints with mechanical instability.
With his guidance, the students’ 2014 Senior Capstone project undertook an ambitious to a challenging problem. They were able to design a customizable three-dimensional tissue-engineering scaffold. Their scaffold supports full thickness osteochondral repairs in joints with mechanical instability.
Dr. Miller was excited to serve as an adviser. He congratulated the students on a well earned Best Business Design Overall award.
To read the complete article on University of Maryland’s website, please click here.
Orthopaedic Research & Articles
October 5, 2015
Beacon Orthopaedics and Sports Medicine Encourages Orthopaedic Research & Articles:
Continuous research and education is a key part for all of the doctors at Beacon. This is very evident in the work and contributions of Dr. Adam Miller. Through research and engineering, improvements in technology, new treatment options are developed for various conditions. By contributing to Orthopaedic Research & Articles, Dr. Miller is able to offer innovative and advanced care.
Below are several links to articles or research to which Dr. Miller has collaborated or contributed. Select any of the links in this section to learn more about Dr. Miller’s academic research.
- Delasotta LA, Orozco F, Miller AG, Post Z, Ong A. Distal femoral fracture during primary total knee arthroplasty. J Orthop Surg (Hong Kong). 2015;23(2).
- Raikin SM, Miller AG, Daniel J. Recurrence of Hallux Valgus: A Review. Foot Ankle Clin. 2014.
- Orozco F, Post ZD, Baxi O, Miller A, Ong A. Fibrosis in hepatitis C patients predicts complications after elective total joint arthroplasty. J Arthroplasty. 2014;29(1):7-10.
- Miller AG, Schon LC. Fixation of Midfoot and Forefoot Fractures. Techniques in Orthopaedics. 2014;29(1):24-32.
- Miller A, Raikin SM. Lateral Ankle Instability. Operative Techniques in Sports Medicine. 2014;22(4):282-9.
- Miller AG, Raikin SM, Ahmad J. Near-Anatomic Allograft Tenodesis of Chronic Lateral Ankle Instability. Foot & ankle international / American Orthopaedic Foot and Ankle Society [and] Swiss Foot and Ankle Society. 2013 Jun 14. Epub 2013/06/19.
- Miller AG, McKenzie J, Greenky M, Shaw E, Gandhi K, Hozack WJ, et al. Spinal Anesthesia: Should Everyone Receive a Urinary Catheter? The Journal of Bone & Joint Surgery. 2013;95(16):1498-503.
- Miller AG, Daniel JN. Achilles tendon pathology associated with tophaceous gout infiltration. Current Orthopaedic Practice. 2013;24(1):103-4.
- Garras DN, Durinka JB, Bercik M, Miller AG, Raikin SM. Conversion Arthrodesis for Failed First Metatarsophalangeal Joint Hemiarthroplasty. Foot & ankle international / American Orthopaedic Foot and Ankle Society [and] Swiss Foot and Ankle Society. 2013 Apr 23. Epub 2013/04/25.
- Miller AG, Slenker N, Dodson CC. Terrible triad of the shoulder in a competitive athlete. Am J Orthop (Belle Mead NJ). 2012 May;41(5):228-9. Epub 2012/06/21.
- Miller AG, Purtill JJ. Total knee arthroplasty component templating: a predictive model. J Arthroplasty. 2012 Oct;27(9):1707-9. Epub 2012/05/29.
- Miller AG, Purtill JJ. Accuracy of digital templating in total knee arthroplasty. Am J Orthop (Belle Mead NJ). 2012 Nov;41(11):510-2. Epub 2013/02/23.
- Miller AG, Margules A, Raikin SM. Risk factors for wound complications after ankle fracture surgery. J Bone Joint Surg Am. 2012 Nov 21;94(22):2047-52. Epub 2012/11/23.
- Miller AG, Bercik MJ, Ong A. Nonagenarian hip fracture: treatment and complications. J Trauma Acute Care Surg. 2012 May;72(5):1411-5. Epub 2012/06/08.
- Garras DN, Hansen PL, Miller AG, Raikin SM. Outcome of modified Kidner procedure with subtalar arthroereisis for painful accessory navicular associated with planovalgus deformity. Foot Ankle Int. 2012 Nov;33(11):934-9. Epub 2012/11/08.
- Bercik MJ, Miller AG, Muffly M, Parvizi J, Orozco F, Ong A. Conversion total hip arthroplasty: a reason not to use cephalomedullary nails. J Arthroplasty. 2012 Sep;27(8 Suppl):117-21. Epub 2012/05/29.
- Aynardi M, Miller AG, Orozco F, Ong A. Effect of work-hour restrictions and resident turnover in orthopedic trauma. Orthopedics. 2012 Nov;35(11):e1649-54. Epub 2012/11/07.
- >Parvizi J, Miller AG, Gandhi K. Multimodal pain management after total joint arthroplasty. J Bone Joint Surg Am. 2011 Jun 1;93(11):1075-84. Epub 2011/06/10.
- Miller AG. Weighing your future job options in today’s market. Am J Orthop (Belle Mead NJ). 2011 Nov;40(11):E241-2. Epub 2012/01/21.
- Miller AG, Swank ML. Dermabond efficacy in total joint arthroplasty wounds. Am J Orthop (Belle Mead NJ). 2010 Oct;39(10):476-8. Epub 2011/02/04.
- Swank ML, Miller AG, Korbee LL. Transition Zone Failure in Patients Undergoing Instrumented Lumbar Fusions from L1 or L2 to the Sacrum. 2007.