
Ankle Sprains
October 5, 2015
Rolled, Twisted and Turned: How to Get Back on the Court After Ankle Sprains
Rolled, twisted, and turned: three words that no one wants to associate with their ankles. All are common descriptions of ankle sprains. Ankle injuries can result in fracture, tendon injury, or most commonly an ankle sprain. There are an estimated one to 10 million acute ankle injuries in the United States on a yearly basis with fractures accounting for only 15 percent. (Berkowitz & Fierstein, 2011).
 Ankle sprains are typically evidenced by pain and swelling in the ankle. A popping or snapping sensation may be felt and the person may have difficulty with bearing weight. Bruising is also common but may not be visible until hours or days after injury. The good news about ankle sprains is that most resolve with rest and support, however, what differentiates the ankle sprain that can be “walked off” almost immediately from the sprain which requires immobilization or surgical intervention? What type of support and treatment result in faster returns to activity or work?
Ankle sprains are typically evidenced by pain and swelling in the ankle. A popping or snapping sensation may be felt and the person may have difficulty with bearing weight. Bruising is also common but may not be visible until hours or days after injury. The good news about ankle sprains is that most resolve with rest and support, however, what differentiates the ankle sprain that can be “walked off” almost immediately from the sprain which requires immobilization or surgical intervention? What type of support and treatment result in faster returns to activity or work?
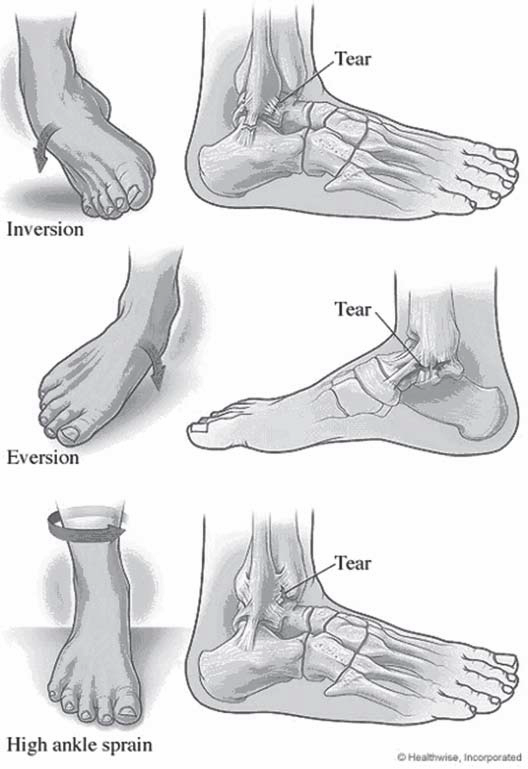
The ankle is a complex joint where the tibia (shin) and fibula (small bone of the outer leg) meet the talus (upper-most bone of the foot.) This joint is stabilized by three main ligament complexes. The most commonly injured are those of the outside or lateral ankle. These include the anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and posterior talofibular. These are typically injured when someone lands or rolls on the outside of their foot causing what is known as a forced inversion injury.
The inner ankle is stabilized by a number of ligaments known collectively as the deltoid ligaments. These are more commonly injured when a person rolls or land on the inner foot causing a forced eversion injury. This type of injury is also more likely to cause a fracture. The third set of ligaments is between the two bones of the lower leg and is known collectively as the syndesmosis. A high ankle sprain refers to injury to this syndesmosis.
Ankle sprains are typically diagnosed by a good history and physical examination. The physician will ask about the mechanism of injury and symptoms from the time of injury. They will examine the ankle to see where it is most tender and stress the ligaments to assess for any instability. They should also check the function of nerves and blood vessels that travel to the foot for any possible injury. X-rays may be necessary to rule out a fracture.
The Ottawa Foot and Ankle rules are a commonly used guideline for obtaining x-rays in acute injury. These guidelines state that x-rays should be obtained if the patient has tenderness over certain bone structures (medial malleolus, fifth metatarsal, or novicular), or if the patient is unable to bear weight immediately after injury or at time of examination. These are tailored to use in the emergency department and other guidelines may be used by an orthopedist or primary care provider. In those with persistent pain, an MRI to further evaluate the soft tissues may be needed.
Ankle sprains range in severity much like any other injury. Some are minor enough that even hours after injury the patient feels better. Others may last for weeks or require surgical intervention. The degree of pain and dysfunction is generally attributed to the amount of damage to the ligament or ligaments. Different grading systems can describe these in different manners.
No matter the severity of the sprain, the first measures of treatment are typically conservative. RICE (rest, ice, compression, and elevation), therapy can be helpful initially to help with pain relief and control of acute swelling. Anti-inflammatories such as ibuprophen or naproxen have also been traditionally used for pain and inflammation control. This has become more controversial in recent years as newer studies suggest that NSAID use may delay healing as inflammation is the body’s natural response to an injury in that it causes chemical signals in the body to recruit nutrients and growth factors to the site of injury. It is theorized that blocking this initial inflammation may lead to delayed healing.
Another traditional form of treatment for ankle sprains has been splinting or rigid bracing for immobilization. More recently there has been a rise in functional treatment for Grade I and Grade II sprains. Functional treatment typically consists of support with a lace-up or semi-rigid brace coupled with early physical therapy exercises to restore motion and strength. Ivins, et. al, showed people returning to sports 4.6 days sooner and work 7. 1 day sooner with functional treatment. Another study (Kerkhoff’s et. al, 2009), shows that more patients return to sport 4.88 days faster, and return to work 8.23 days faster. In general, they found that more people returned to sport in the long run.
Ankle therapy includes general range of motion as well as strengthening about the ankle. This is often combined with something referred to as proprioceptive training. Proprioception is the ability for a person to sense where they are in space. This is what allows us to catch objects in the air or step up and sown meeting the floor without falling. The nerve fibers that give us this sense are often impaired due to the ankle sprain often requiring retraining to prevent further injury from new falls or awkward positions.
Common ankle exercises for both treatment and prevention of an ankle sprain include range of motion exercises, which can simply be performed using a cloth or towel wrapped around the foot with the ends firmly in both hands. Gently pull the towel toward the face and hold for 15-30 seconds. This can be varied by also pulling with an inward roll of the ankle and outward roll of the ankle. These can be repeated 3-5 times. Also, you can perform a standing calf stretch by bending the knees while standing with their heels on the floor. Another creative way to work on ankle range of motion is to spell the alphabet with the great toe by moving the ankle through different planes.
Once you have full range of motion, strengthening exercises can be started to help prevent re-injury. Simple exercises can include pushing downward, upward, inward and outward on an immovable object holding each for 5 second for 10 sets. Then dynamic (moving), strengthening using the other foot, rubber tubing or weights can include the same motions, but instead of pushing and holding, this includes fully contracting the muscles over 1 second followed by taking 4 seconds to relax the ankle for three sets of 10 repetitions. Using the toes to pick up small objects and walking forward and backward on toes and heels are also common strengthening exercises.
Proprioceptive training is typically started when the patient can weight bear without much pain. This can be as simple as heel raises and toe raises or as involved as using a wobble board as well as walking on different surfaces (Berkowitz & Fierstein, 2011). Proprioception is also improved with single leg balance and using a jump rope. Formal physical therapy is often needed to initiate different exercises although most can be done at home. A good strengthening program helps facilitate your return to the court.