
What is a Biceps Tendon Rupture and How is it Fixed?
March 17, 2017
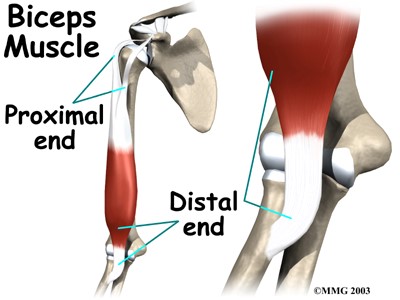
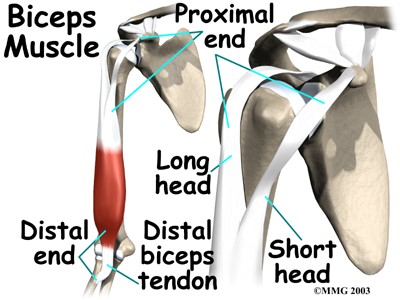
The biceps muscle group (biceps brachii) is made up of two heads, the long head and the short head. The muscles originate at the shoulder and insert on the radius (short bone in the forearm). The main function of the biceps brachii is to supinate the forearm (pretend like you are holding a cup of soup in the palm of your hand; this position is called “supination”). The second function of the biceps brachii is to flex (bend) the elbow. Rupture of the biceps tendon can occur proximally (at the shoulder) or distally (at the elbow). Ruptures commonly occur when there is an unexpected force applied to the bicep muscle such as attempting to catch something or someone when they fall. Most ruptures occur when the elbow is in a flexed position. Some people may feel or hear a “pop” when the tendon separates from the bone.
How is a Biceps Tendon Rupture diagnosed?
Ruptures of the biceps tendon can usually be diagnosed through history and physical exam. Observation of the injured extremity may reveal significant bruising and swelling, as well as physical deformity. The physical deformity associated with biceps ruptures is termed popeye deformity. The deformity is due to the tendon retracting toward the muscle belly causing a large bulge. X-rays may be ordered to rule out an associated avulsion fracture. An MRI may also be ordered to aid in visualizing the amount of damage sustained to the muscle, tendon, and bone.
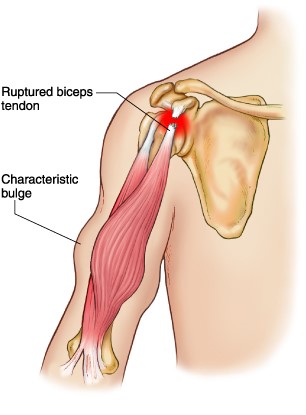
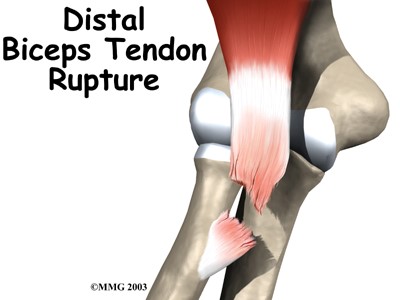
Image courtesy of mdguidelines.com Image courtesy of eorthopod.com
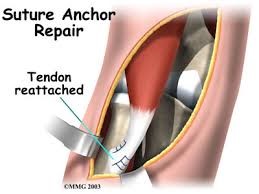
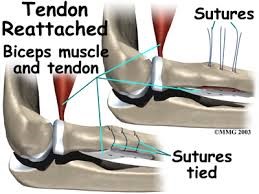
What is Biceps Tendon Repair surgery?
Distal biceps tendon ruptures typically require surgical fixation to restore range of motion and strength to the elbow. This procedure is an open surgical procedure which can be performed on an outpatient basis. The goal is to reattach the tendon to the radius bone using either sutures or anchor with sutures.
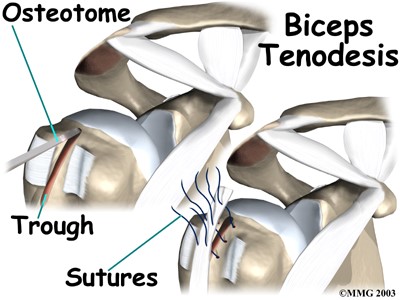
Proximal biceps tendon ruptures can be treated conservatively with physical therapy and anti-inflammatories. Surgery is considered when a patient continues to have pain despite conservative measures. The biceps tendon is not reattached to its original origin; the biceps is attached to the humerus in a procedure called a “biceps tenodesis.”
Why should I consider Bicep Tendon Surgery?
Distal repair for a biceps tendon rupture should be considered in patients that injure the bicep in their dominant arm, or active individuals. The goal of surgery is to restore strength and endurance to the musculature as well as maintain range of motion in the elbow joint. Without surgery, there is a significant probability that function of the injured extremity will be limited. Proximal bicep tendon repair is considered when conservative measures fail or do not relieve pain.
What are my restrictions after a Bicep Tendon Surgery?
Total healing time for any injury or surgical repair is usually one year. Limitations vary based on distal or proximal repair. Both repairs for a biceps tendon rupture will require the use of a post-operative sling for up to 4 weeks. Physical therapy will begin range of motion and strengthening activities based on protocols established by Dr. Rolf, or your preferred surgeon.
What will be my recovery time?
Distal and proximal bicep tendon repairs are performed as an outpatient surgery. Formal physical therapy can begin within 2 days of surgery. Formal therapy can last 12-16 weeks with gradual progression to a home exercise program. Most patients are able to return to normal activity, without restriction, 14-20 weeks after surgery. The variable wide range of return to activity is based on a distal or proximal bicep repair.
What are the risks of surgery to repair a biceps tendon rupture?
Complications associated with bicep tendon repair are rare. Common risks associated with a distal repair include: decreased strength, decreased nerve sensation, and decrease range of motion at the elbow. Common risks associated with proximal repair include: decreased strength, decreased nerved sensation, and decreased range of motion at the shoulder. Both surgical techniques have associated risk of pain, infection, and slow wound healing.

Written By: Lisa Osterbrock, PA-C, ATC
Edited By: Robert Rolf, M.D.
Images courtesy of proactivept.com, eorthopod.com, and mdguidelines.com.