
Achilles Injuries
October 5, 2015
Preventing Achilles Injuries: What can go wrong on the court?
Most people are familiar with the great story of Achilles who was dipped into the River Styx to become invincible. Unfortunately, Thetis held him at the ankle and so is born the “Achilles heel.” According to Homer’s Illiad, Achilles was slain when Paris shot an arrow into his heel. Fortunately, flying arrows are rare in today’s world, but that does not mean that you are immune to Achilles injuries on the court.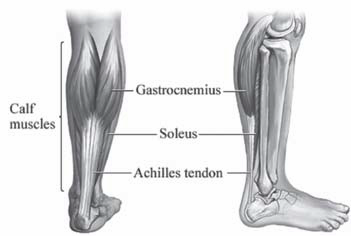
The Achilles tendon inserts on the back of the heel (or the calcaneus). It is comprised of two muscles (the gactrocnemeus and the soleus) which merge to become one tendon. It becomes round and then flattens about 4 cm. proximal to the heel. There are essentially four Achilles injuries that can arise with the tendon: Achilles tendinitis and tendinosis, paratenonitis, insertional tendinitis and Achilles ruptures.
Achilles Tendonitis
Achilles tendonitis is a condition when the Achilles is irritated and inflamed. There is a relatively avascular zone in the Achilles tendon that is roughly 2-6 cm. for the insertion of the Achilles into the heel. It is a common injury in recreational athletes and occurs when there is overuse of the tendon that causes inflammation leading to pain and swelling. When the condition is chronic, it leads to Achilles 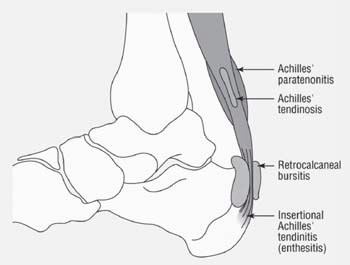 tendinosis. With tendinosis, there are microscopic tears within the tendon. The paratenon is a sheath that envelopes the tendon. It can become inflamed with repetitive strain or overuse. The tendon may also be thickened. The pain improves with rest and is aggravated with activity. It tends to be associated with overuse and is not a precursor to Achilles ruptures. Insertional tendinitis is characterized by inflammation and pain surrounding the point where the tendon inserts into the heel. This can lead to partial tearing or rupturing of the tendon. A person will complain of tenderness directly over the Achilles insertion into the heel and can make weightbearing difficult. The tendon can become hardened and thickened. Surgery may be necessary for those cases recalcitrant to nonoperative treatment such as rest, cross-training, anti-inflammatories, stretching, and physical therapy.
tendinosis. With tendinosis, there are microscopic tears within the tendon. The paratenon is a sheath that envelopes the tendon. It can become inflamed with repetitive strain or overuse. The tendon may also be thickened. The pain improves with rest and is aggravated with activity. It tends to be associated with overuse and is not a precursor to Achilles ruptures. Insertional tendinitis is characterized by inflammation and pain surrounding the point where the tendon inserts into the heel. This can lead to partial tearing or rupturing of the tendon. A person will complain of tenderness directly over the Achilles insertion into the heel and can make weightbearing difficult. The tendon can become hardened and thickened. Surgery may be necessary for those cases recalcitrant to nonoperative treatment such as rest, cross-training, anti-inflammatories, stretching, and physical therapy.
Achilles Tendon Ruptures
Achilles tendon ruptures can occur in the substance of the tendon (in the avascular zone) or they can occur where the tendon avulses off the calcaneus. They are up to 12 times more common in men than women and usually result from noncontact injuries where the load to the Achilles exceeds the strength of the tendon. This can result from mechanisms such as a forceful push-off of the foot with an extended knee (jumping or sprinting), sudden unexpected ankle dorsiflexion, or violent dorsiflexion of a plantar-flexed foot.
Many times, a person may feel like they got kicked in the back of the heel by someone. The immediate pain is shortlived, but people will notice the inability to push the heel off the ground when walking. There may be swelling and/or bruising. Sometimes, a person may notice a palpable defect in the tendon. It is usually difficult to walk. When a physician squeezes the calf in the normal ankle, the foot will dorsiflex or flex down toward the ground. When the same test is done in the injured leg, there is no movement at the ankle. This is called a positive Thompson test. Achilles ruptures are almost always diagnosed clinically, but when there is uncertainty, an MRI is an excellent test to evaluate the integrity of the Achilles tendon.
Despite recent attention to surgical treatment of Achilles ruptures, the decision to treat these injuries surgically versus nonoperatively remains controversial. Nonoperative management is historically associated with a high risk of Achilles rerupture, ranging from 13 to 30%, but without wound complications. Operative management of Achilles tendon ruptures results in a lower re-rupture rate (0 to 6%), earlier mobilization, and better return to sports, but with the risk of higher wound complications (up to 21%). Recent studies suggests an infection rate that is much lower.
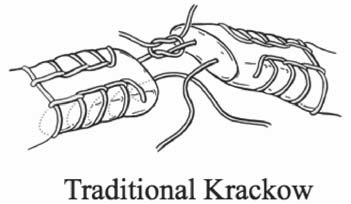
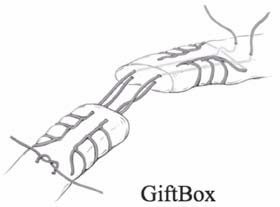
The goal of surgical management is early mobilization to maximizes healing potential. This requires strong suture material and a sound technique. Two such techniques include the Krackow suture and the “Giftbox” technique. as described by
Labib, et al.
After surgery, the repair is splinted for up to two weeks with no weight bearing. Thereafter, the heel is placed in a boot with heel lifts that are removed over the next month. Weight bearing usually begins around two weeks, although this may vary depending on the surgeon.
Achilles injuries occur as a result of being in the right situation at the wrong time. That is, the force applied to the tendon is stronger than the tendon can withstand. Sometimes, that just cannot be prevented. Achilles tendon injuries such as tendinitis, insertional tendinitis, tendidnosis, and paratenonitis typically respond well to nonoperative management.
Prevention of Achilles Injuries:
As people age, calf and Achilles tightness is almost inevitable due to several reasons. First, as we become more sedentary, we have less daily stretch of the calf muscles and Achilles tendons. There is also age-related decrease in the elasticity of the Achilles tendon. Finally, higher-heeled shoes put the Achilles tendon in a shortened position. A good stretching and strengthening program is the best way to prevent Achilles injuries.
Achilles tendon stretching will result in satisfactory relief in better than 90% of the people suffering from Achilles pain. Some
people require as little as 3 weeks to see improvement while others may need upwards of 5-6 months to break through a long standing Achilles contracture. The heel stretching protocol is outlined below in detail. In the beginning, the amount you stretch will vary due to pain or soreness of the Achilles. Be sure to stretch both feet.
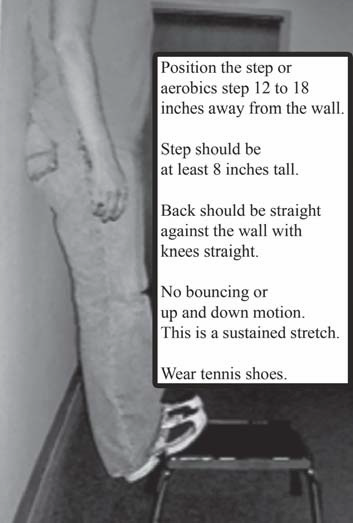
First of all, you will need a step to stand on with a wall for support. A routine step lift works extremely well. With your back against the wall and your knees straight, place the balls of your feet on the step and slowly relax your ankles, letting your heels go downward (see figure). You should not be gripping the step with your toes. If you are in the correct position, you should feel a pulling or tightness in your upper calf muscle, just below the knee. This should be tolerated until slight pain is felt.
For best results, do the stretch three times per day, gradually increasing the amount of time. You may need to stay at the same amount of hang time for a few days. Increase your time gradually, maxing out at three minutes. This is a gradual process and be patient. If you go right to three minutes, you may cause yourself more pain. Be Patient!
 Week I – 15 seconds, 3 times/day
Week I – 15 seconds, 3 times/day
Week II – 30 seconds, 3 times/day
Week III – 1 minute, 3 times/day
Week IV – 1 1/2 minutes, 3 times/day
Week V – 2 minutes, 3 times/day
Week VI – 2 1/2 minutes, 3 times/day
Week VII – 3 minutes, 3 times/day